

Background: The thin face is one in which the perception of the width to length ratio is disproportionate. This could be that the vertical length of the face is excessive by forehead or chin lengths even though the width of the face is normal. It could also be that the vertical facial length is normal but the width of the cheeks and jawline are too narrow.
More frequently a face is perceived as thin, regardless of the bone structure, because of fat loss or lipoatrophy. Most commonly the fat loss occurs in the temples and the submalar cheek area due to buccal fat loss. In some people this does not occur by fat loss but by natural lack of fat development. Their face is thin and has always been so.
In treating the congenitally narrow face where both bone and soft tissue augmentation is needed, options include injectable fillers, fat injections and implants. Patients may try injectable fillers initially and this can certainly provide some benefit. Ultimately because they are not permanent and may produce an improved but still inadequate result, more permanent treatment options are pursued.
 Case Study: This male had a thin face with temporal narrowing and midface hypoplasia. He had been getting injectable fillers (Radiesse) into the midface of 2cc per side. While providing some volume improvement it had an inadequate effect although it did provide a roadmap of where the augmentation of the midface was desired.
Case Study: This male had a thin face with temporal narrowing and midface hypoplasia. He had been getting injectable fillers (Radiesse) into the midface of 2cc per side. While providing some volume improvement it had an inadequate effect although it did provide a roadmap of where the augmentation of the midface was desired.
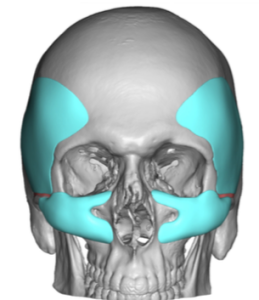
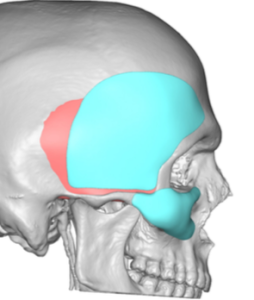
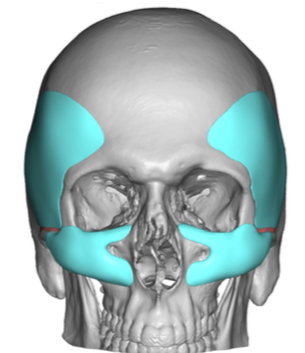
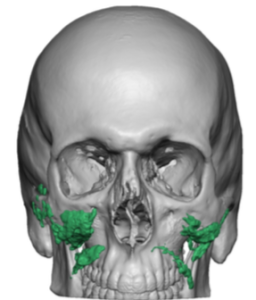
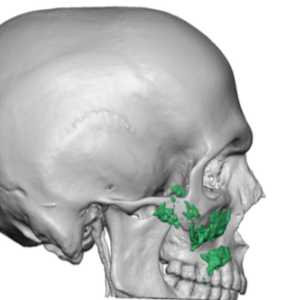
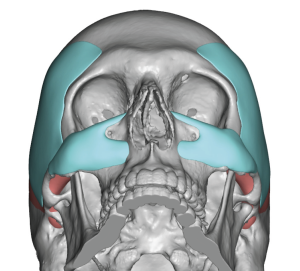 Using his 3D CT scam custom extended temporal-forehead implants were designed to fill in the temporal hollows as well as cross over onto the forehead to correct he associated bony forehead narrowing. Custom midface implants were designed that covered the infraorbital rim, anterior cheek and onto the concavity of the maxilla. The implants encircled the infraorbital rim.
Using his 3D CT scam custom extended temporal-forehead implants were designed to fill in the temporal hollows as well as cross over onto the forehead to correct he associated bony forehead narrowing. Custom midface implants were designed that covered the infraorbital rim, anterior cheek and onto the concavity of the maxilla. The implants encircled the infraorbital rim.

 In placing these custom implants the goal is accurate placement but with minimal visible scarring to do so.
In placing these custom implants the goal is accurate placement but with minimal visible scarring to do so.


 Under general anesthesia and through postauricular incisions aided by a small incision just behind the frontal hairline, the custom extended temporal-forehead implants were introduced and positioned. A small screw was used to secure its position at the frontal hairline position.
Under general anesthesia and through postauricular incisions aided by a small incision just behind the frontal hairline, the custom extended temporal-forehead implants were introduced and positioned. A small screw was used to secure its position at the frontal hairline position.


 The custom midface implants were introduced and placed through a combined lower eyelid and intraoral incisions. Getting the implants around the infraorbital nerve as well as making sure they fit properly on the infraorbital rims required a dual incisional access.
The custom midface implants were introduced and placed through a combined lower eyelid and intraoral incisions. Getting the implants around the infraorbital nerve as well as making sure they fit properly on the infraorbital rims required a dual incisional access.
The thin face can be a combination of lack of facial fat as well as skeletal deficiencies. Injectable synthetic fillers may produce some volume improvements but are often inadequate. The thin face rarely does well with fat injections due to poor retention. Properly design custom facial implants for temporal hollows and midface deficiencies can be an effective approach with the key to not making the implants too big. In the thin face large surface area coverages do no require as much implant thicknesses as one may think.
Case Highlights:
1) The thin face is often a combination of a lack of facial fat and a more narrow bone structure.
2) Facial fullness can be created through a combination of temporal and a specific form of cheek (infraorbital-malar) augmentation using custom implant designs.
3) Placement of such custom facial implants can be done with discreet incisions from behind the ear and through the lower eyelid.
Dr. Barry Eppley
Indianapolis, Indiana