


Background: The five surfaces of the skull are prone to a wide variety of surface contour irregularities. In theory all five surfaces could be equally affected by these shape deformations but that is not so. Three of the five skull surfaces are completely bony but the sides are covered with muscle. Since almost all skull contour issues are bony in origin the three bony surfaces (forehead, top and back of head) are where all such irregular shapes can be found.
Of these three bony surfaces the back of the head is by far the ,most affected by various aesthetic shape deformities. This is due to its exposure to more external forces during its development than the other surfaces of the skull. The occipital bone, which makes up a significant part of the back of the head, is one of the thickest of all the skull bones and has a large number of soft tissue attachments both externally and internally.
As a result of these influences there are some basic or classic bony shape deformations to the back of the head. One such deformity is the prominent midline occipital knob at the level of the nuchal ridge line. (the lowest part of the visible back of the head) While most people have one they are usually small and invisible. But in the shaved or short haired male even small knobs can become visible. Another extremely common back of head deformity, and the most common, is various amounts of flattening or lack of convex projection. If an occipital knob is present it will be more visible as the slope of the head above it is more forward.
The side of the head has fewer shape issues and some of these may be a bit arbitrarily aesthetic and not a real abnornality. This is seen in the wide or excess convexity to the side of the head. It is uniquely different from all other skull contour concerns because it is has a soft tissue basis and not a bony one.The temporal muscle contributes more to the width of the side of the head than the bone. Subtotal muscle removal is a very effective method of head width reduction and does not cause any functional issues.
Case Study: This young male had multiple skull shape issues from a small occipital knob to an upper flat back of the head. He was also bothered by the wider shape to the sides of his head.
 Under general anesthesia and in the prone position a 1 cm incision was made over the occipital knob which allowed its complete reduction.
Under general anesthesia and in the prone position a 1 cm incision was made over the occipital knob which allowed its complete reduction.
 Then through an incision higher up at the bottom end of the flat area, 20 grams of bone cement was prepared, passed through the incision and shaped until it was set.
Then through an incision higher up at the bottom end of the flat area, 20 grams of bone cement was prepared, passed through the incision and shaped until it was set.

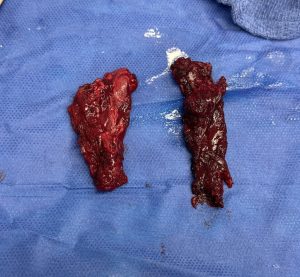 Changing from the prone to supine position posterior temporal muscle removal was done through post auricular incisions.
Changing from the prone to supine position posterior temporal muscle removal was done through post auricular incisions.
Three drains were placed and a head dressing applied, all of which were removed the following day.

 When seen four days postop he looked remarkably good as I would have expected much more swelling to still be present. The improvement in the shape of the back of the head could be seen in profile from the augmentation at the upper back of the head and small occipital knob reduction.
When seen four days postop he looked remarkably good as I would have expected much more swelling to still be present. The improvement in the shape of the back of the head could be seen in profile from the augmentation at the upper back of the head and small occipital knob reduction.

 While his head width was not dramatically excessive, its immediate reduction could also be seen….which is surprising at just 4 days after surgery.
While his head width was not dramatically excessive, its immediate reduction could also be seen….which is surprising at just 4 days after surgery.
Key Points:
1) Two contour issues can occur simultaneously on the back of the head such as in this case upper flattening and an occipital knob.
2) An occipital knob reduction and upper back of head augmentation can be concurrently performed through small overlying incisions.
3) Bone cements can be successfully used for very small skull augmentation but are done for economic reasons and not because they offer a superior aesthetic outcome.
4) Temporal reductions can also performed with any back of the head surgery but it requires a change from the prone to supine intraoperative positioning.
Dr. Barry Eppley
World-Renowned Plastic Surgeon