


Background: A common method of aesthetic jaw augmentation in my practice, although not well known at all to many, is combining an osteotomy with implants. In this specific method a bony genioplasty is done for the anterior third of the jaw and custom implants are used for the remaining two-thirds of the jaw behind it. This approach is used when the amount of dimensional changes in the chin are significant due to the limitations of how much the tight soft tissue chin pad can be pulled over an implant.
In placing implants on the chin, it is first necessary to detach the soft tissues to create the tissue pocket for the implant. Then the implant is placed and the soft tissue chin pad must be pulled over the implant and a relatively non-tight closure must be done. (the same applies whether it is a submental or intraoral incisional approach. When the need is for significant chin augmentation the potential limitation of the soft tissue chin pad will be eventually encountered. In bringing the chin horizontally forward more than 10mms it may be difficult, but not impossible, to get the soft tissue chin pad pulled back over it with a competent closure. But when a vertical increase is involved with a horizontal augmentation, getting the soft tissue chin pad back over the bone becomes more challenging and in some cases impossible. This where the traditional bony genioplasty has an advantage over an implant…it does not have this soft tissue chin pad limitation as the soft tissue attachments on the inferior edge of the bone remains intact.
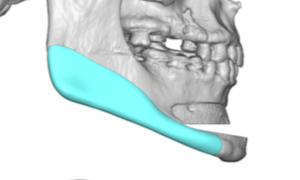
Unlike the bony genioplasty the rest of the jaw behind it does not have the same soft tissue limitations. Besides the fact that only implants can make changes behind the chin, implants along the jawline particularly in the vertical dimension (lengthening) can be effectively done. Custom implant designs are needed to have the anterior end of the implant blend into the repositioned chin bone for a complete jawline augmentation.
 Case Study: This male has an existing chin implant which did little to improve the shape of his chin. He desired to have a more complete jawline augmentation to improve what was largely a vertical deficiency of the lower third of his face. In these vertical deficiencies it is always greatest at the chin. Using predictive imaging it was determined that he needed 8mm vertical lengthening and 7mms horizontal lengthening. This was deemed too much in which to use an implant for this degree of chin augmentation change.
Case Study: This male has an existing chin implant which did little to improve the shape of his chin. He desired to have a more complete jawline augmentation to improve what was largely a vertical deficiency of the lower third of his face. In these vertical deficiencies it is always greatest at the chin. Using predictive imaging it was determined that he needed 8mm vertical lengthening and 7mms horizontal lengthening. This was deemed too much in which to use an implant for this degree of chin augmentation change.

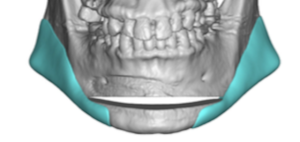
 A combined bony genioplasty and custom jawline implants was used to achieve his desired aesthetic jaw augmentation changes.
A combined bony genioplasty and custom jawline implants was used to achieve his desired aesthetic jaw augmentation changes.

 His six month result shows good improvement in his jawline, particularly in the vertical dimension of the chin.
His six month result shows good improvement in his jawline, particularly in the vertical dimension of the chin.

 When it comes to using an implant for jaw augmentation the limiting factor is the chin. This is not so evident in the horizontal dimension but becomes a significant factor for vertical lengthening of the chin. As a guideline I use the concept of ’12’ as to what ca be achieved with an implant in the chin. That number refers to the combination of horizontal and vertical dimensional changes. Any number over 12 should be done by a bony genioplasty and will avoid a large implant load on the soft tissue chin pad.
When it comes to using an implant for jaw augmentation the limiting factor is the chin. This is not so evident in the horizontal dimension but becomes a significant factor for vertical lengthening of the chin. As a guideline I use the concept of ’12’ as to what ca be achieved with an implant in the chin. That number refers to the combination of horizontal and vertical dimensional changes. Any number over 12 should be done by a bony genioplasty and will avoid a large implant load on the soft tissue chin pad.
Case Highlights:
1)With large chin augmentation changes a sliding genioplasty is a more effective and safer approach due to the limitations of the soft tissue chin pad.
2) Augmenting the jawline behind the repositioned chin bone can be done with custom implants to create a smooth jawline.
3) Merging the jawline implant with the chin bone advancement is more difficult than it looks as there is a need for the anterior end of the jawline implant to be visualized and secured to the chin.
Dr. Barry Eppley
World Renowned Plastic Surgeon