


Background: A midface deficiency affects the middle third of the face from the infraorbital rims down to the maxillary alveolus. In its classic presentation the patient has a class III malocclusion or underbite but that may not be evident if prior orthodontic correction and orthognathic surgery has been done. Despite a corrected occlusion the midface will still have an aesthetic deficiency from undereye hollows superiorly down to a recessed nasal base inferiorly.
Correction of the deficient midface above the alveolus is usually treated by implant augmentation. Standard implants that exist for the midface include cheek, tear trough and paranasal/premaxillary implants. They can be effective for modest deficiencies but lack the ability to create an overall connected midface augmentation effect. Only custom designed implants can address all deficient areas of the midface by essentially expanding the infraorbital rim-maxillary bony contours.
For the midface custom implants can be designed to cover all of the midface or just select parts of it. Some patients start right from the beginning and treat the entire problem with an implant design known as the midface mask. Others start out with augmenting one area of the midface with the realization that a more complete midface effect is desired later…as the following case illustrates.
 Case Study: This young male previously had custom infraorbital-malar implants to treat undereye hollows and flat cheeks. While successful he came to realize that his nasal base was also flat/recessed. His 3D CT scan showed recessed nasal base and a very deep and concise maxillary shape.
Case Study: This young male previously had custom infraorbital-malar implants to treat undereye hollows and flat cheeks. While successful he came to realize that his nasal base was also flat/recessed. His 3D CT scan showed recessed nasal base and a very deep and concise maxillary shape.
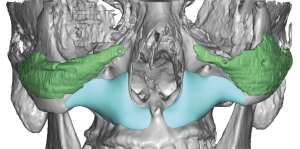
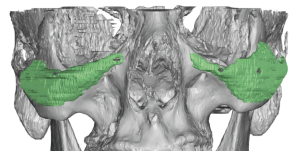
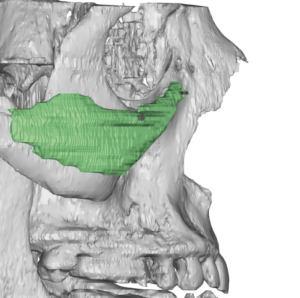
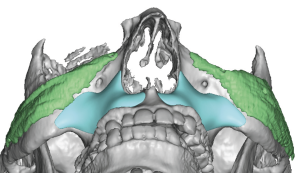
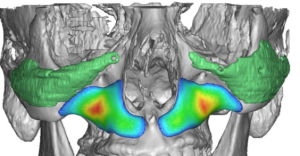 Custom implants were designed to augment the pyriform aperture across the entire maxilla up onto the lower surface of the zygoma, getting close to but not completely touching the infraorbital-malar implants. The thickest part of the implant was in the depth of the maxillary concavity at 9mms as seen in the color mapping of the implant’s thickness.
Custom implants were designed to augment the pyriform aperture across the entire maxilla up onto the lower surface of the zygoma, getting close to but not completely touching the infraorbital-malar implants. The thickest part of the implant was in the depth of the maxillary concavity at 9mms as seen in the color mapping of the implant’s thickness.
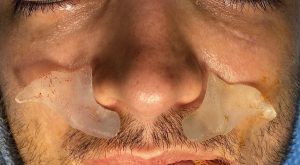


 Through intraoral vestibular incisions subperiosteal pockets were created and the implants placed and secured with a single small screw to upper posterior zygomatic buttress. (making sure the screw tips do not enter the maxillary sinus)
Through intraoral vestibular incisions subperiosteal pockets were created and the implants placed and secured with a single small screw to upper posterior zygomatic buttress. (making sure the screw tips do not enter the maxillary sinus)
 While paranasal augmentation is typically thought of as just enhancing the base of the nose it is often part of an overall mdface deficiency/flatness. Leaving the immediate paranasal location just lateral to it is the canine fossa and the rest of the concave maxillary surface. The more concave the maxilla is the more recessed the midface can be. While standard paranasal implants fit snugly around the base of the nose they do not venture far out onto the rest of the maxilla. This is why some standard paranasal implants will create a palpable bump under the nasolabial fold area due to the abrupt transition of the raised edge of the implant and the deeper canine fossa. The custom paranasal-maxillary implant avoids this aesthetic problem by extending to cover the entire maxillary surface.
While paranasal augmentation is typically thought of as just enhancing the base of the nose it is often part of an overall mdface deficiency/flatness. Leaving the immediate paranasal location just lateral to it is the canine fossa and the rest of the concave maxillary surface. The more concave the maxilla is the more recessed the midface can be. While standard paranasal implants fit snugly around the base of the nose they do not venture far out onto the rest of the maxilla. This is why some standard paranasal implants will create a palpable bump under the nasolabial fold area due to the abrupt transition of the raised edge of the implant and the deeper canine fossa. The custom paranasal-maxillary implant avoids this aesthetic problem by extending to cover the entire maxillary surface.
Case Highlights:
1) A paranasal deficiency is often part of an overall maxillary midface deficiency.
2) Augmenting a maxillary midface deficiency requires an extended paranasal-maxillary implant design.
3) Placed intraorally a custom paranasal-maxillary implant is secured by screw fixation to the zygomatic body.
Dr. Barry Eppley
Indianapolis, Indiana