

Background: The jawline and neck are connected by more than just anatomic proximity. The amount of projection of the chin and the length of the jawline affects the appearance of the neck profile. The shorter the chin projection the more obtuse the cervicomental neck angle becomes. Conversely the greater the chin projection the less obtuse/more acute the cervicomental angle will appear. The best results in any lower facial reshaping must look at the relationship between the chin projection and neck angle and determine if just one or both areas need to be treated for the most pleasing lower facial shape.
In considering augmentation of very short chins one usually has to move beyond implants and consider the sliding genioplasty procedure. The value of the sliding genioplasty in short chins, beside not placing a large implant load on the end of the chin bone, is its effect on the shape of the neck. Through the bony attachments of the geniohyoid and the anterior digastric muscle to the back of the chin, these muscles are pulled forward as the chin bone is advanced. In addition there is also the push of the bone on the insertion of the platysma muscle into the soft tissue chin pad. Collectively these create a muscle lengthening effect which helps extend the horizontal axis of the cervicomental angle and may even elevate the hyoid bone a bit. A chin implant sitting on top of the chin bone does not have such a muscular lengthening effect.
In managing the neck with any form of chin augmentation the options are liposuction, submentoplasty and a necklift/lowerfacelift. Since many patients that specifically undergo chin and/or jawline augmentation are on the younger side the neck considerations are either liposuction or submentoplasty. A submentoplasty elevates the effect of liposuction by also removing deeper central neck fat as well as doing a midline platysma muscle plication. This has a more profound effect on the cervicomental angle.
Case Study: This male presented for chin augmentation to improve a lifelong shorter chin/no neck appearance. Through computer imaging it was established that, while he wanted a stronger chin, he did not want it too strong. In other words don’t bring the chin out to the classic vertical line dropped down from the lip position. While this may be the ideal chin position for some it can often appear to be too much for the patient who has lived with a short lower face for their whole life. This is a phenomenon I call transitional shock or facial disrecognition. This is the value that preoperative computer imaging has in avoiding this type of ‘over corrected’ result.



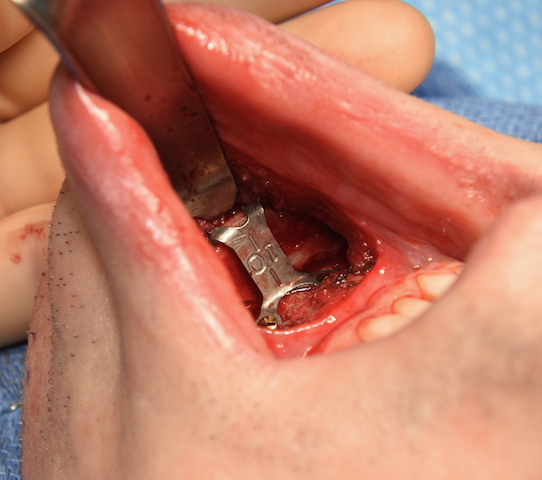
 Under general anesthesia an intraoral sliding geniopasty was performed with a 10mm pure horizontal bone advancement. This brought the back edge of the advanced chin bone out the very front edge of the chin bone above it. Tissue back bone chips were used to graft the bony step off created by the advanced bone movement. Then from a submental incision the neck was treated by liposuction, direct central subplatysmal fat removal and midline platysma muscle plication.
Under general anesthesia an intraoral sliding geniopasty was performed with a 10mm pure horizontal bone advancement. This brought the back edge of the advanced chin bone out the very front edge of the chin bone above it. Tissue back bone chips were used to graft the bony step off created by the advanced bone movement. Then from a submental incision the neck was treated by liposuction, direct central subplatysmal fat removal and midline platysma muscle plication.
While the ideal treatment for a very short chin patient is orthognathic surgery with at least a sagittal split lower jaw advancement, in adults this may not be the extent of treatment they want to pursue. The aesthetic camouflage for such lower jaw deficiencies is a major chin augmentation procedure. A debate can be had between a large chin implant and a sliding genioplasty. As long as the goal is not to have a more square chin shape I would prefer to make such an augmentation effect buying one’s own tissues which is associated with fewer potential complications. When combined with a submentoplasty the diametric movements create the best lowe face reshaping as is possible.
Case Highlights:
1) In the adult with a really short chin a sliding genioplasty is usually the preferred chin augmentation procedure.
2) Short chin/lower jaws are associated with a very obtuse cervicomental angle which is best treated by a submentoplasty procedure.
3) Combining a sliding genioplasty with a submentoplasty is the most extreme diametric lower facial/neck change that can be done from an aesthetic standpoint.
Dr. Barry Eppley
Indianapolis, Indiana