

Background: The chin implant is the most common form of lower facial augmentation but it has its limits. Since the soft tissue chin pad must be released to allow an implant to be placed on the bone the stretch of these overlying soft tissues poses a restriction on implant size. As a result chin implants work best on modest chin deficiencies where the amount of augmentation needed is 10 mm or less in projection.
But when the lower jaw is under developed the chin recession is more significant and will exceed more than 10mms of needed chin augmentation. There are numerous clinical signs that indicate such chin projection severities from a deep labiomental fold, a proclined lower lip, lack of vertical chin height, excessive submental fullness despite a good weight and a chin that is angled backward. While such patients are not usually good candidates for a chin implant they often get the procedure in lieu of jaw surgery or a sliding genioplasty due to either patient or what the surgery knew or felt comfortable doing.
In severe chin recession short of major jaw surgery the treatment of choice is a sliding genioplasty. Such chin bone movement is capable of more than 10 mm of horizontal projection and is not limited by the overlying soft tissue chin pad. As the chin is often tilted backwards and elongated the sliding genioplasty can also bring the chin forward to either maintain its current vertical lengthen it or even shorten it. Despite the superiority of a bone procedure instead of an implant it is not uncommon to see such a patient who sends had a chin implant initially and desires an improved result. This raises the question as to whether the implant should be removed and completely replaced with a sliding genioplasty or keep the implant intact and move the bone forward with the implant attached. That choice is influenced by how much additional chin augmentation is needed, the position of the existing implant on the bone and whether any change is needed in vertical height.
Case Study: This male had a significant chin deficiency which was initially treated by a 7mm extended chin implant placed intraorally with three screw fixation. While he liked the result when it was early and after surgery and swollen once that resolved he did not feel that much improvement. By external measurements he needed at least another 10 to 12 mm of horizontal chin augmentation.
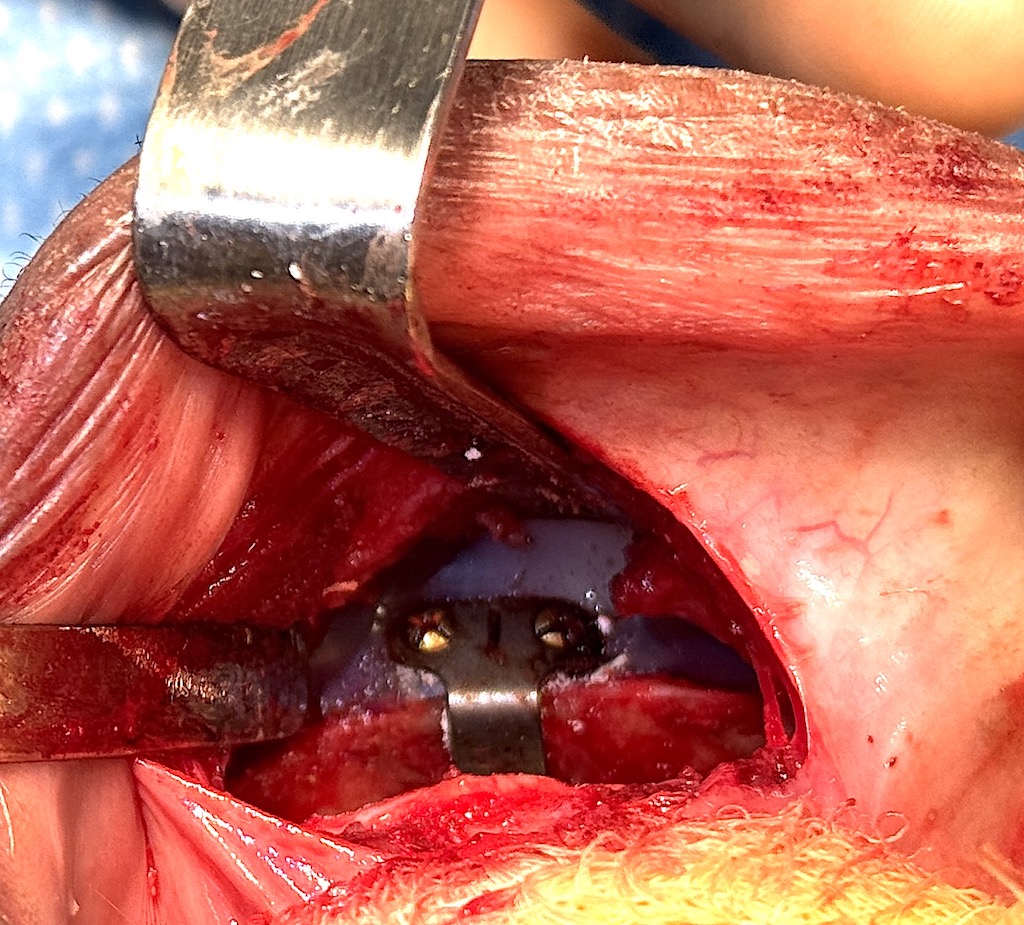
 Under general anesthesia and through an intraoral approach the chin implant was exposed. Along the top of the implant a full thickness bone cut was made and the chin bone with the implant attached down fractured. Using a 12mm titanium step plate the chin bone was advanced and secured with screws. The plate was bent with an upward tilt to prevent any additional chin lengthening.
Under general anesthesia and through an intraoral approach the chin implant was exposed. Along the top of the implant a full thickness bone cut was made and the chin bone with the implant attached down fractured. Using a 12mm titanium step plate the chin bone was advanced and secured with screws. The plate was bent with an upward tilt to prevent any additional chin lengthening.

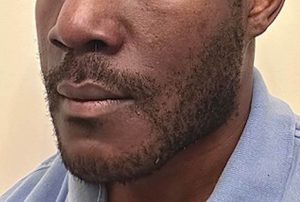
 His postoperative result compared to where he was before the chin implant showed a dramatic change in the shape and projection of his lower face.
His postoperative result compared to where he was before the chin implant showed a dramatic change in the shape and projection of his lower face.

The progression of before any surgery, after the chin implant and after the sliding genioplasty showed the incremental improvement in chin projection.

 In this two stage implant-osteotomy chin augmentation sequence the patient had 19mms of added lower facial projection. This exceeded what either technique could do alone.A sliding genioplasty can be successfully done with a chin implant in place based on where the implant is on the bone. If the implant is low enough a bone cut above it can be safely done staying well below the tooth roots and the mental nerve foramen. At the level of the osteotomy the screws of the fixation plate will likely have to go through the implant as well to secure the plate to the bone.
In this two stage implant-osteotomy chin augmentation sequence the patient had 19mms of added lower facial projection. This exceeded what either technique could do alone.A sliding genioplasty can be successfully done with a chin implant in place based on where the implant is on the bone. If the implant is low enough a bone cut above it can be safely done staying well below the tooth roots and the mental nerve foramen. At the level of the osteotomy the screws of the fixation plate will likely have to go through the implant as well to secure the plate to the bone.
Key Points:
1) A sliding genioplasty can be performed with an indwelling implant for maximal chin augmentation.
2) When performing a sliding genioplasty over a chin implant the implant needs to be low enough on the bone for a safe level of the bone cut.
3) With an implant on the advanced chin bone one has to be careful that the chin does not become excessively long so the genioplasty fixationplate must benbent upward so the advanced segment is shortened.
Dr. Barry Eppley
World-Renowned Plastic Surgeon