

Background: Ons of then most common aesthetic ear procedures is a setback otoplasty to reduce protruding ears. While a wide variety of techniques have been described to do this operation the fundamental concept is that the ear is set back closer to the side of the head by either creating or increasing the antihelical fold of the outer ear cartilage. Getting the ideal amount of ear setback through cartilage suturing/excision is as much an art form as it is a science on either side not to mention symmetry between the two ears.
In setback otoplasty, besides an ideal result, under- and overcorrection of the ear protrusion are possible adverse aesthetic outcomes. Undercorrection is the more easily improvable of the two as more setback can always be done. Overcorrection of an otoplasty, however, is viewed as the more challenging to improve due to scar, loss of cartilage memory and possible loss of cartilage structure if excision was performed as part of the setback.The most common area of the ear to be pulled back too far is the central third. It is in this area of the ear where the most extensive cartilage work can be done due to the large conchal bowl. Both suture and cartilage excision can be done in this area and it is also viewed as the most important part of the ear to setback.
Overcorrection of the middle third of the ear is seen as a loss of the outer helical rim behind the antihelical fold in the front view. This is known historically as a ‘telephone’ deformity but anatomically the ear is folded back too much as a smooth continuous outer helical rim appearance is lost. While a simple release of the back of the ear would seem effective this only works if done shortly after the surgery…and only if cartilage has not been excised. Once scarred in only a supported ear release will be effective.
Case Study: This male had a setback otoplasty 9 months previously. The exact techniques to do so were unknown. He felt it was over corrected with the middle part of the ear pulled back too far.
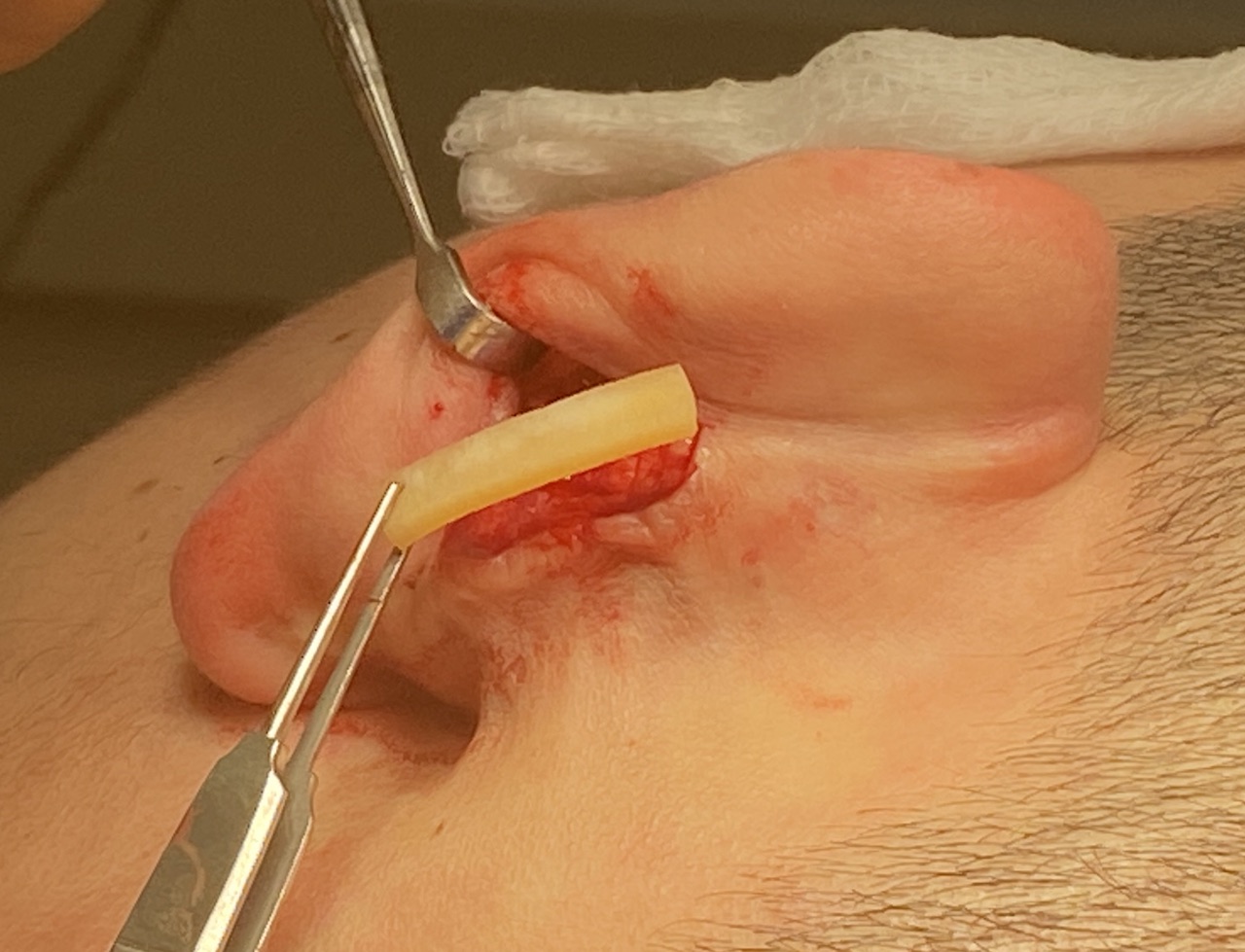
 Under local anesthesia the central part of the scar on the back of the ear was opened and the fold of the ear exposed. The two sides of the fold (helical rim and antihelix) was released to create a space between between. Permanent blue sutures were seen aplenty if the released area.
Under local anesthesia the central part of the scar on the back of the ear was opened and the fold of the ear exposed. The two sides of the fold (helical rim and antihelix) was released to create a space between between. Permanent blue sutures were seen aplenty if the released area.
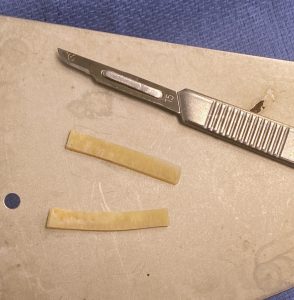

 A cadaveric rib cartilage graft was dethwed and cut into two strips. The rib grafts were then used as wedges int the space created by theifold release. The incision was closed over the graft in two layer with resorbable sutures.
A cadaveric rib cartilage graft was dethwed and cut into two strips. The rib grafts were then used as wedges int the space created by theifold release. The incision was closed over the graft in two layer with resorbable sutures.

 The immediate results showed the improved appearance of the ears with a visible and smooth outer helical rim from top of the ear down to the earlobe.
The immediate results showed the improved appearance of the ears with a visible and smooth outer helical rim from top of the ear down to the earlobe.
A supported ear release means that an interpositional graft is used to hold the released cartilage in its new position. A variety of materials could be used to do so from metal plates to dermal grafts to rib grafts. I have used them all and all can work. Short of using the patient’s own rib graft, which few patients understandably would be willing to have such a harvest, a cadaveric rib graft seems the most biologic. (cartilage into cartilage)
Case Highlights:
1) Disruption of the outer helical rim after a setback otoplasty can have an adverse perception of the aesthetic outcome.
2) The most common area of helical rim distortion is in the middle third of the ear due to overcorrection.
3) Improving an over corrected setback otoplasty requires the combination of a release AND placement of an interpositional cartilage graft to prevent relapse of the expanded ear position. (subtotal reverse otoplasty)
Dr. Barry Eppley
World-Renowned Plastic Surgeon