

Background: The sliding genioplasty is one of the most well known of all the facial bone osteotomies. It is a unique lower facial osteotomy because it has no functional impact on jaw movement. The chin is a pure aesthetic aspect of the lower jaw that is not responsible for any biomechanical load transfer. It is cut and moved for aesthetic purposes only and can alter the chin in three dimensions although the horizontal forward advancement is its most known movement historically.
The chin is a central projecting structure in which a horizontal advancement is moving a down fractured segment but into space so to speak. The fixation hardware used for most sliding genioplasties is placed centrally due to the midline access. As the chin bone is fixated centrally it is prone to asymmetries which can be due to differences in the length and angle of the osteotomy lines on each side as well as magnifications of any existing bone asymmetries.
When such asymmetries of the chin exist after the bone has been moved, there are two corrective approaches. The bone can be recut and repositioned or the position of the chin is maintained and the outer edges of the chin bone reshaped through either addition or subtraction. In most cases of sliding genioplasty asymmetries the latter is usually what would be effective.

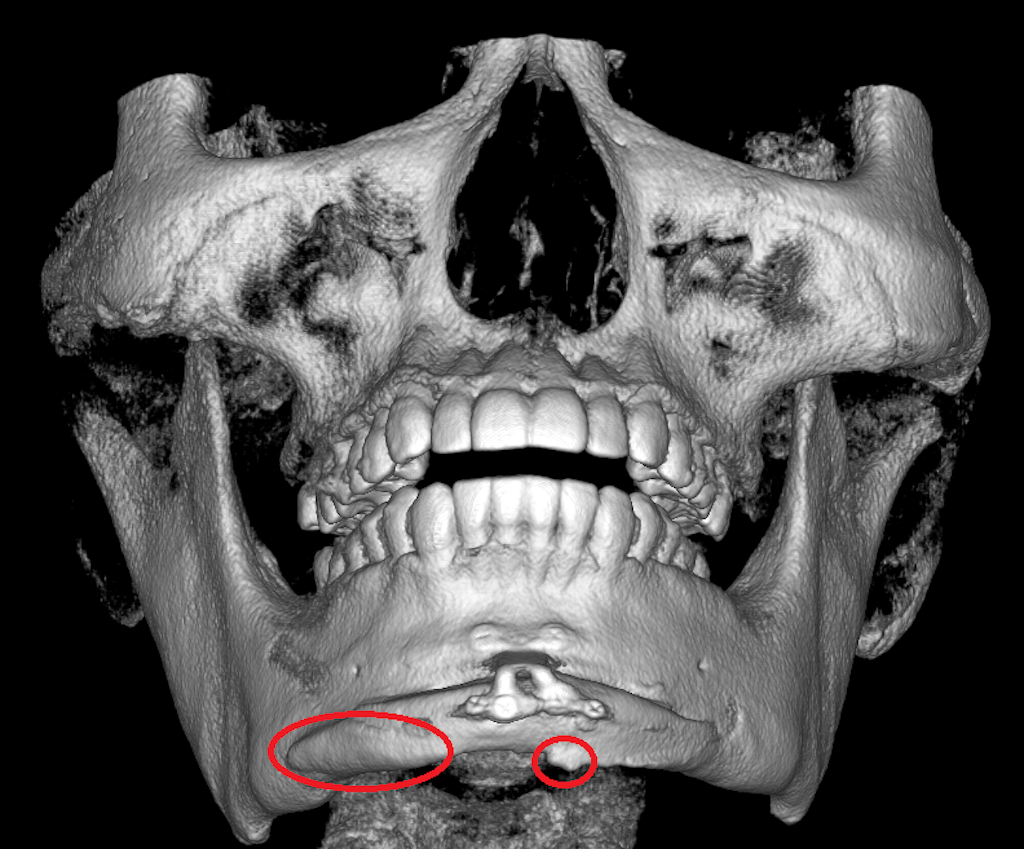
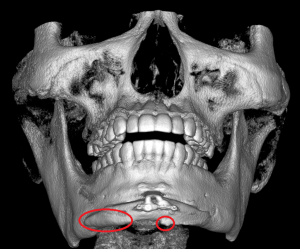 Case Study: This male had a 12mm sliding genioplasty done to replace a large chin implant one. While aesthetically successful in terms of achieving good chin projection there was some asymmetry of the bone shape that appeared after all the swelling went down. A 3D CT scan showed one primary area of the asymmetry, a more protrusive right side, and a smaller bump of bone on the left side.
Case Study: This male had a 12mm sliding genioplasty done to replace a large chin implant one. While aesthetically successful in terms of achieving good chin projection there was some asymmetry of the bone shape that appeared after all the swelling went down. A 3D CT scan showed one primary area of the asymmetry, a more protrusive right side, and a smaller bump of bone on the left side.
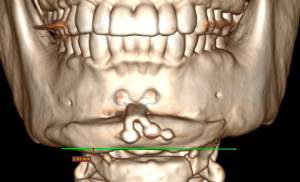
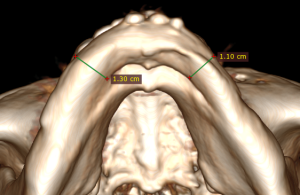 Measurements showed that the horizontal difference between the two chin sides was a 1.93mm increased length on the right side and a 2mm anterior protrusion on the right side as well.
Measurements showed that the horizontal difference between the two chin sides was a 1.93mm increased length on the right side and a 2mm anterior protrusion on the right side as well.
 Under general anesthesia and through an existing submental scar (from the 1st chin implant) the right inferior border was shaved as well as the excessive anterior projection of the right chin bone reduced. The screws were removed from the lower legs of the fixation plate as their heads were palpable.
Under general anesthesia and through an existing submental scar (from the 1st chin implant) the right inferior border was shaved as well as the excessive anterior projection of the right chin bone reduced. The screws were removed from the lower legs of the fixation plate as their heads were palpable.
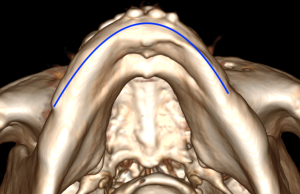 One cause of chin asymmetry after a sliding genioplasty is due to a tilt or rotation of the repositioned chin bone. This can happen if the osteotomy cuts differ in length or angulation between the two sides or the front end of the fixation plate where the chin bone is attached develops a slight tilt. This is not rare as the size of the incision used is very small compared to the total length of the osteotomy line. The back ends of the bone cuts are not well seen making the cut and are not seen at all once the bone is repositioned. The other cause is performing a sliding genioplasty when jaw asymmetry exists…which turns out to be the cause when looking at the 3D CT scan postop. With jaw asymmetry the chin is not evenly shaped on both sides. Many times this asymmetry is not seen before surgery as it is mild or it may be masked by an indwelling chin implant as in this case. Even with fairly symmetric bone cuts the chin asymmetry becomes more apparent as the chin bone becomes more projected.
One cause of chin asymmetry after a sliding genioplasty is due to a tilt or rotation of the repositioned chin bone. This can happen if the osteotomy cuts differ in length or angulation between the two sides or the front end of the fixation plate where the chin bone is attached develops a slight tilt. This is not rare as the size of the incision used is very small compared to the total length of the osteotomy line. The back ends of the bone cuts are not well seen making the cut and are not seen at all once the bone is repositioned. The other cause is performing a sliding genioplasty when jaw asymmetry exists…which turns out to be the cause when looking at the 3D CT scan postop. With jaw asymmetry the chin is not evenly shaped on both sides. Many times this asymmetry is not seen before surgery as it is mild or it may be masked by an indwelling chin implant as in this case. Even with fairly symmetric bone cuts the chin asymmetry becomes more apparent as the chin bone becomes more projected.
It is not surprising that a few millimeters of tilt in the chin bone can become so apparent given that it creates the solitary central projection of the lower face.
Case Highlights:
1) The sliding genioplasty procedure is prone to asymmetries of the advanced chin segment.
2) More modest sliding geniopalsties asymmetries can be treated by a submental shave technique if reductive bone changes are the asymmetry correction.
3) A 3D CT scan is needed to make the proper assessment and measurements for how to make the reductive chin changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon