

Background: While the back of the head as an aesthetic unit is a single skull surface the bones that make it upon are not. The back of the head is comprised of the paired upper parietal bones and inferiorly by the single occipital bone. They are merged together by the inverted Y suture lines. As a result there are a variety of different aesthetic back of the head shape problems which can occur from these three bones.
Back of the head, often called occipital which is technically inaccurate, shape issues fall into vertical and horizontal types. For example, plagiocephaly or back of head asymmetry may be thought of as a horizontal or side to side shape issue. Conversely an occipital bun or knob disrupts the vertical shape of the back of the head as seen in profile. While both types have some cross over dimensional changes associated with them you get the general concept of these two back of the head shape deformity categories.
In the vertical back of head shape deformations, while many occur as a result of one problem, occasionally you can have two different shape issues combined. When their adverse effects are diametric more profound shape changes can occur. Equally relevant is that the corrective procedures needed get a more desired shape are also diametric in their effects. (augmentation vs reduction)
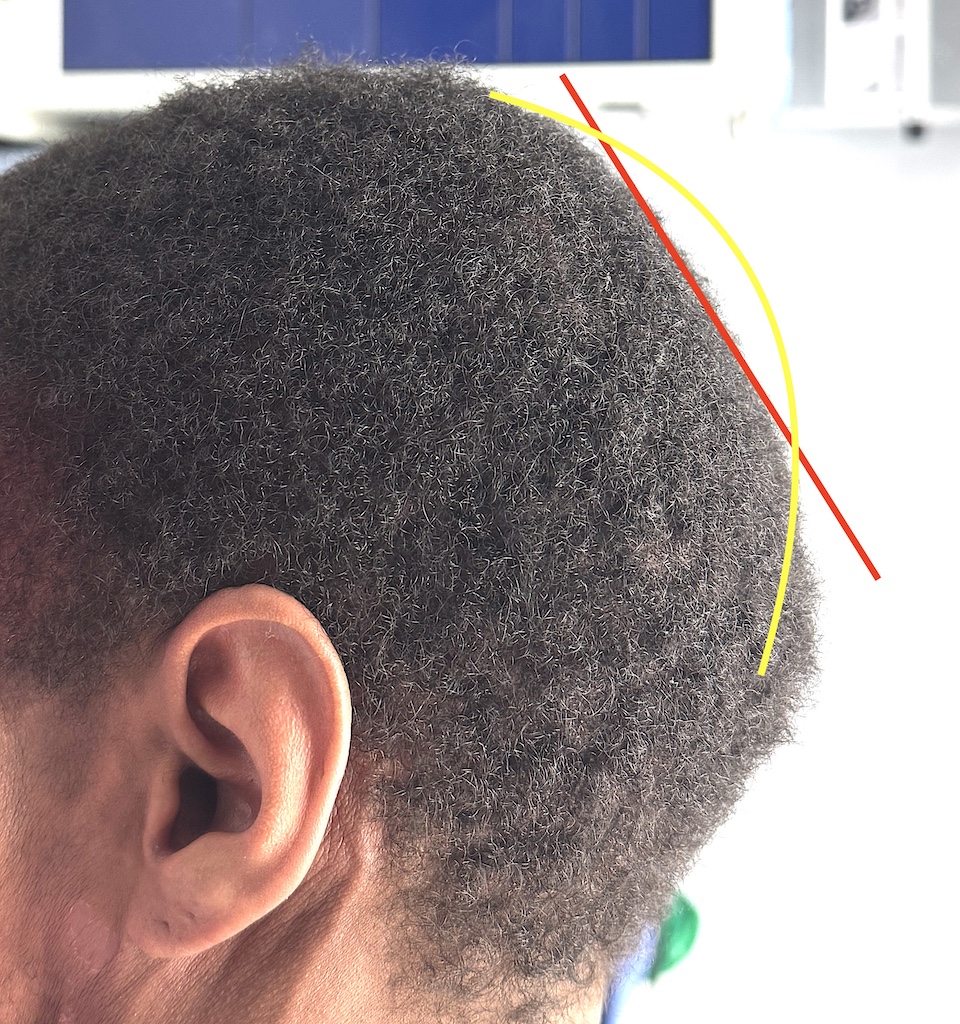
 Case Study: This young male had concerns about the back of his head. The central upper part was dipped in and the central bottom part was protruded. By examination the bottom protrusion was a prominent occipital knob (inion) and top dip was a posterior fontanelle crater-like indentation. Neither one was excessively large but put together created a backward slope (red line) vs a more desired round shape. (green line)
Case Study: This young male had concerns about the back of his head. The central upper part was dipped in and the central bottom part was protruded. By examination the bottom protrusion was a prominent occipital knob (inion) and top dip was a posterior fontanelle crater-like indentation. Neither one was excessively large but put together created a backward slope (red line) vs a more desired round shape. (green line)
 Under general anesthesia and in the prone position a small scalp incision was initially made over the occipital knob where it was burred down to a less projected but rounded shape that went inward at its bottom edge.
Under general anesthesia and in the prone position a small scalp incision was initially made over the occipital knob where it was burred down to a less projected but rounded shape that went inward at its bottom edge.

 Then a second small scalp incision was made at the bottom edge of the posterior fontanelle dip and the scalp elevated out of the crater indentation. Using 30 grams of PMMA bone cement the drop was filled in and contoured externally as it set into a firm smooth shape.
Then a second small scalp incision was made at the bottom edge of the posterior fontanelle dip and the scalp elevated out of the crater indentation. Using 30 grams of PMMA bone cement the drop was filled in and contoured externally as it set into a firm smooth shape.
Both incisions were closed after placing a single drain connecting them and exiting out in the neck.

 The immediate effect of the procedures provides a positive improvement in the shape of the back of his head.
The immediate effect of the procedures provides a positive improvement in the shape of the back of his head.

 When seen the next day for drain removal and before going home the positive improvement was confirmed in the upright head position.
When seen the next day for drain removal and before going home the positive improvement was confirmed in the upright head position.
When treating a dual aesthetic problem on a skull surface an important decision is incision management. Do you make one longer incision between the two or make two smaller incisions more directly over them. That decision will depend on the magnitude of the contour deformities to be treated. But in two smaller type skull surface irregularities it made the most sense to treat them as if they were independent surgeries with two smaller incisions.
Key Points:
1) The back of the head can have a diametric shape problem requiring combined augmentation and reduction techniques.
2) A flatter/depressed upper back of the head and a prominent lower back of the head is the most common dual vertical shape problem.
3) In smaller skull defects like the posterior fontanelle indentation bone cement augmentation can be effective as the most economic augmentation solution.
4) Two smaller scalp incisions can be used to treat both back of the head reshaping needs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon