

Background: The soft spots on a baby’s head are well known and are its most distinguishing features. These open areas between the developing skull bones , known as fontanelles, total six in number but the most visible are the anterior and posterior ones. The anterior fontanelle is the largest of the two and closes between 12 to 24 months of age. The posterior fontanelle is much smaller, is more triangular in shape and closes much sooner within two months after birth.
Closure of these fontanelles represents a union of four bone surfaces meeting across the gap and fusing with bone. While this consistently occurs in almost all patients how thick this bony closure becomes can lead to a variety of aesthetic skull shape deformities around it. In some cases a shallow bony crater forms directly over the center of the fontanelle creating what I call a posterior fontanelle dip or dimple. Presumably this comes from a bone thickness that is thinner in the center than the surrounding skull areas.
In other cases a generalized skull flattening occurs over the posterior fontanelle region which may represent an early closure of the fontanelle gap…somewhat like a craniosynostosis but not exactly. The bone growth is restricted a bit around it leading to decreased projection. Conversely brain growth pushes more anteriorly leading to a moderate frontal bulging. Putting the two together the head shape in profile becomes slanted forward due to the lack of posterior projection and too much upper forehead projection.
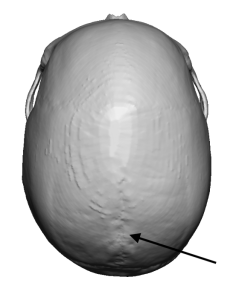 Case Study: This male had a flattened posterior fontanelle skull flattening and some moderate frontal bossing. His 3D CT scan showed that clearly as well as multiple foramina over the depressed area at the back end of the sagittal suture line.
Case Study: This male had a flattened posterior fontanelle skull flattening and some moderate frontal bossing. His 3D CT scan showed that clearly as well as multiple foramina over the depressed area at the back end of the sagittal suture line.
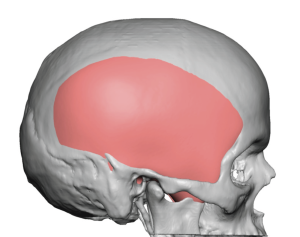
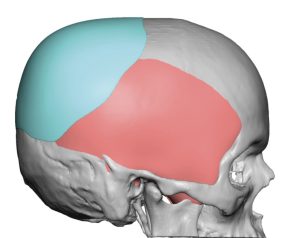 Using his 3D scan a custom skull implant was design to build up the flattened posterior fontanelle area as well as blend in with the rest of the surrounding skull to give a rounder shape. Its maximum projection was 10mm with a 103cc implant volume.
Using his 3D scan a custom skull implant was design to build up the flattened posterior fontanelle area as well as blend in with the rest of the surrounding skull to give a rounder shape. Its maximum projection was 10mm with a 103cc implant volume.

 Under general anesthesia and in the supine position the custom skull implant was placed through a curved scalp incision over the upper back of the head. Multiple linear perfusion holes with a 4mm dermal punch were placed in a vertical and horizontal orientation where the skull implant could be seen through the incision. This would help with both implant orientation once placed under the scalp as well as to help maneuver it around using the ends of a clamp into the holes. Once placed into position the scalp incision was closed over a drain with multilayer resorbable sutures.
Under general anesthesia and in the supine position the custom skull implant was placed through a curved scalp incision over the upper back of the head. Multiple linear perfusion holes with a 4mm dermal punch were placed in a vertical and horizontal orientation where the skull implant could be seen through the incision. This would help with both implant orientation once placed under the scalp as well as to help maneuver it around using the ends of a clamp into the holes. Once placed into position the scalp incision was closed over a drain with multilayer resorbable sutures.

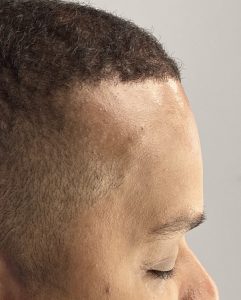 Then switching to the forehead a small incision behind the frontal hairline was used to access the bony forehead. A high speed burring reduction technique was used through a side to side tunnel approach to reduce the frontal bossing by 3 to 4mm maximum at the most projection central forehead area. The amount of forehead reduction could be appreciated in profile intraoperatively.
Then switching to the forehead a small incision behind the frontal hairline was used to access the bony forehead. A high speed burring reduction technique was used through a side to side tunnel approach to reduce the frontal bossing by 3 to 4mm maximum at the most projection central forehead area. The amount of forehead reduction could be appreciated in profile intraoperatively.

 When seen the next day for head dressing and drain removal the correction of the froward sloping head shape in profile could be seen to be improved to a more normal shape. The upper forehead sloped slightly backward and the posterior fontanelle region had more projection with a rounder shape.
When seen the next day for head dressing and drain removal the correction of the froward sloping head shape in profile could be seen to be improved to a more normal shape. The upper forehead sloped slightly backward and the posterior fontanelle region had more projection with a rounder shape.
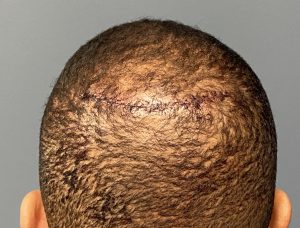
 Both his posterior and frontal scalp incisions are small and will go on to heal with a near invisible appearance particularly given his hair pattern.
Both his posterior and frontal scalp incisions are small and will go on to heal with a near invisible appearance particularly given his hair pattern.

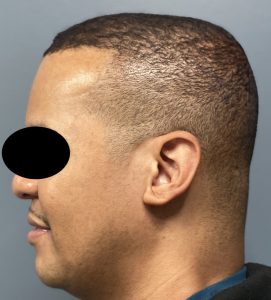 The forward sloping skull shape can arise from a mild growth restriction of the original posterior fontanelle region. Changing its profile shape comes from posterior augmentation and anterior reduction. The augmentation effect will have a greater influence on the skull shape change than the reduction effect. But both are synergistic in terms of head shape profile change.
The forward sloping skull shape can arise from a mild growth restriction of the original posterior fontanelle region. Changing its profile shape comes from posterior augmentation and anterior reduction. The augmentation effect will have a greater influence on the skull shape change than the reduction effect. But both are synergistic in terms of head shape profile change.
Case Highlights:
1) The posterior fontanelle skull deformity is seen as a flat posterior parietal-occipital flattening and an anterior frontal bossing creating a forward tilted head profile.
2) A custom skull implant provides increased posterior projection of the upper back of the head through a small overlying scalp incision.
3) The frontal bossing is reduced concurrently through a small anterior retrohairline incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon