

Background: There are a wide variety of aesthetic head/skull shape deformities. One of the most common one that I see is the peaked head shape. From the front view the midline of the top of the head is the highest point with varying degrees of drop off from the midline of the skull down past the bony temporal line. This creates a V shape with varying degrees of angulation from the apex of the inverted V depending upon the height of the parasagittal/temporal line bone.
The peaked head shape appears by either a heightened sagittal crest and normal parasagittal bone, a normal sagittal crest with a low parasagittal region or a combination of both. In determining which skull area is at fault and requires correction there is a need for computer imaging of the patient’s head shape. In this computer imaging one looks either sagittal crest reduction alone, parasagittal augmentation bone or a combination of both. This is a pure aesthetic choice based on what the patient sees as the best head shape from their perspective based on the different correction method seen by the computer imaging.
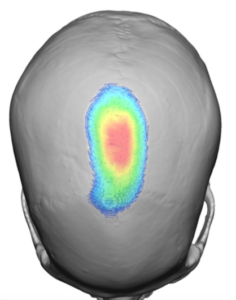
A high sagittal crest runs anteriorly from is connection with the coronal sutures back to the original posterior fontanelle region. Its reduction is usually limited to 5 or 6mms in height reduction. The paired parasagittal region can be deficient from a few millimeters to almost a centimeter in severely slope peaked head shapes. When the parasagittal area is low the bony temporal line will be deficient in height which is the key confirmation of its deficiency. All low parasagittal regions are associated with a flatter upper back of the head (parietal bone) which connects the two sides in the back creating a horseshoe-shape from above. Only a custom skull implant design can provide an adequate correction.
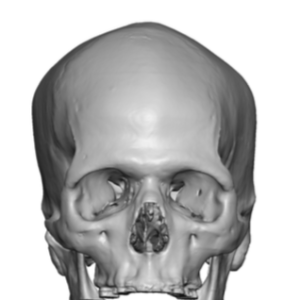
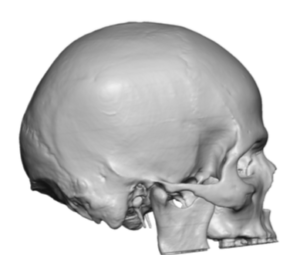
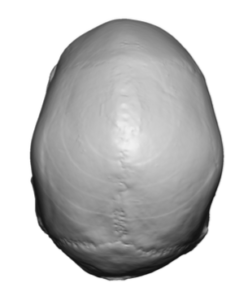 Case Study: This male was bothered by a peaked. head shape which had asymmetric parasagittal regions. He also had a flat upper back of the head which has always bothered him tremendously. A 3D CT scan showed the bony anatomy of his head shape. The flat back of his upper head was asymmetric which corresponded as it wrapped around in the parasagittal region with the flatter right back of the head being associated with the higher right parasagittal region. (a common plagiocephalic finding)
Case Study: This male was bothered by a peaked. head shape which had asymmetric parasagittal regions. He also had a flat upper back of the head which has always bothered him tremendously. A 3D CT scan showed the bony anatomy of his head shape. The flat back of his upper head was asymmetric which corresponded as it wrapped around in the parasagittal region with the flatter right back of the head being associated with the higher right parasagittal region. (a common plagiocephalic finding)
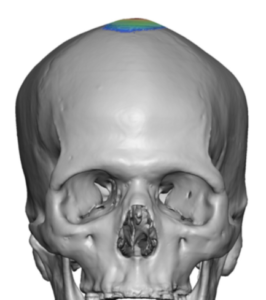
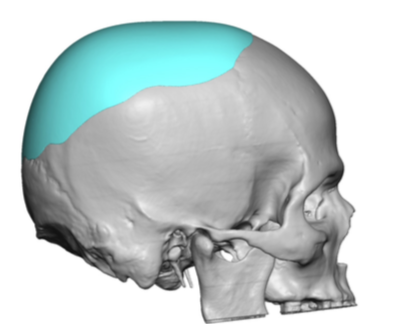
 Using computer imaging of his head shape he opted for a sagittal crest reduction combined with a custom skull implant. A maximal sagittal crest reduction of 4mms was planned.
Using computer imaging of his head shape he opted for a sagittal crest reduction combined with a custom skull implant. A maximal sagittal crest reduction of 4mms was planned.
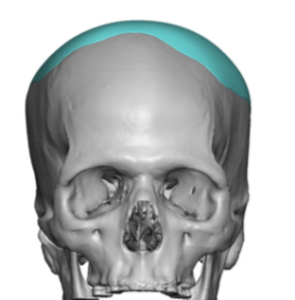
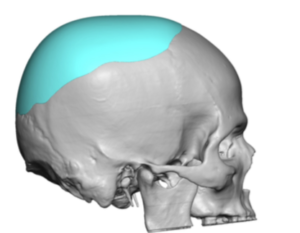
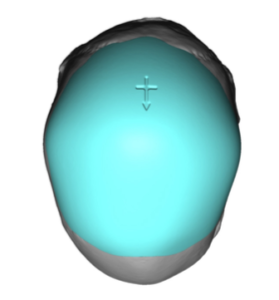 The sagittal ridge reduction was combined with a custom skull implant that crossed over he sagittal crest reduction area (minimal 1mm thickness) to ensure no implant edging on the top of the head. The custom skull implant volume was 100ccs.
The sagittal ridge reduction was combined with a custom skull implant that crossed over he sagittal crest reduction area (minimal 1mm thickness) to ensure no implant edging on the top of the head. The custom skull implant volume was 100ccs.

 Under general anesthesia and through a curved 8cm incision at the back end of the sagittal crest, its bony reduction was done by high speed burring.
Under general anesthesia and through a curved 8cm incision at the back end of the sagittal crest, its bony reduction was done by high speed burring.
Wide subperiosteal undermining developed the pocket for the custom skull implant which was inserted, positioned in the midline and screwed into position.



 The effects of the sagittal rude reduction and skull implant could be appreciated immediately with a more pleasing head shape.
The effects of the sagittal rude reduction and skull implant could be appreciated immediately with a more pleasing head shape.
The peaked head shape is often caused by a combination of sagittal bone excess and parasagittal-parietal bone deficiency. The key corrective element is usually the augmentation created by a custom skull implant design.
Case Highlights:
1) The peaked head shape is morphologically like an inverted V or roof type shape due to either a high sagittal crest, low parasagittal bone or both.
2) Correction of the peaked shape in this case was done by a combination of a sagittal crest reduction (minor) with parasagittal augmentation. (the most significant component)
3) A parasagittal skull deficiency often has a horseshoe-shape that wraps around the sagittal crest with a parietal deficiency in the back.
Dr. Barry Eppley
Indianapolis, Indiana