

Background: There are a variety of raised bony skull areas that present aesthetic deformities which patients request to be reduced. One of the most common is the midline sagittal ridge. While it could occur anywhere along the length of the sagittal suture, and may even involve the entire length of the suture, but most commonly it is the posterior part of the ridge that can be excessively raised. While a prominent sagittal ridge can occur in any gender it is no surprise that is a more common concern in men that have very short hair or a shaved head. (I have yet to see a female for sagittal ridge reduction)
The most important question in considering sagittal ridge reduction is can it be safely done. In other words what is the thickness of the ridge and how much can be removed. While all sagittal ridges I have seen are because the sagittal suture is thickened, and the ridge is always thicker than the parasagittal skull areas at its sides, it is still important to know how much of the ridge in millimeters can be reduced. This can be determined by the thickness of the outer cortical layer and its thickness down to the diploic space. As a general rule if at least 4mms of the ridge can be removed the surgery will usually be worthwhile.

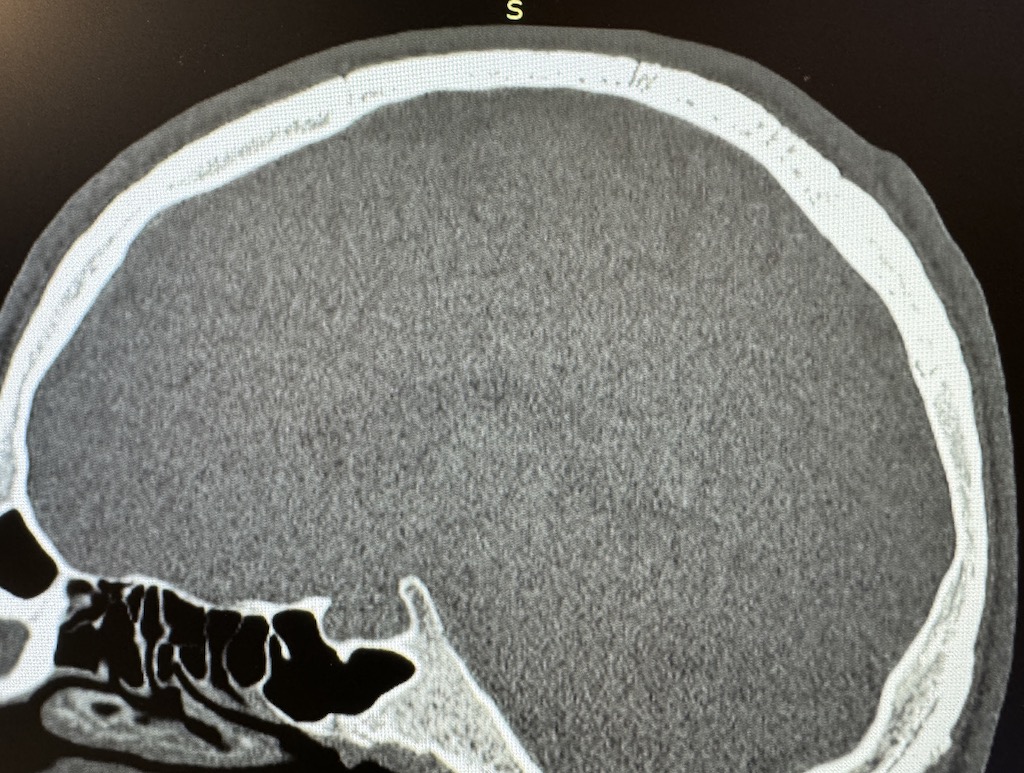
 Case Study: This male desired a posterior sagittal ridge to be reduced. His 2D CT down the middle of the ridge showed good thickness for at least a 4mm reduction. (red line)
Case Study: This male desired a posterior sagittal ridge to be reduced. His 2D CT down the middle of the ridge showed good thickness for at least a 4mm reduction. (red line)
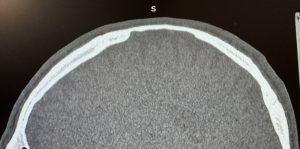 Looking at CT scan slices off of the sagittal ridge in the parasagittal area the thickness of the skull becomes much thinner. In some places too thin to undergo any reduction at all.
Looking at CT scan slices off of the sagittal ridge in the parasagittal area the thickness of the skull becomes much thinner. In some places too thin to undergo any reduction at all.
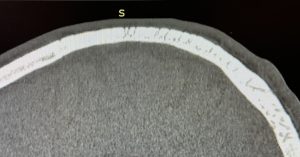 Interestingly in some slices of the CT scan numerous vertical black lines appear which is the fibrous tissue of the suture seen along its serpeginous course down the middle of the skull.
Interestingly in some slices of the CT scan numerous vertical black lines appear which is the fibrous tissue of the suture seen along its serpeginous course down the middle of the skull.
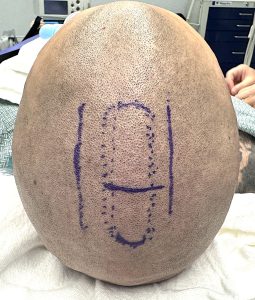
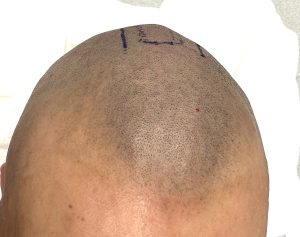 Under general anesthesia the raised portion of the sagittal ridge was marked with the planned incision at its midpoint. The vertical lines on each side of the ridge is the perimeter that the bony reduction should go as this is the area where the skull becomes much thinner. (based on the scan)
Under general anesthesia the raised portion of the sagittal ridge was marked with the planned incision at its midpoint. The vertical lines on each side of the ridge is the perimeter that the bony reduction should go as this is the area where the skull becomes much thinner. (based on the scan)

 Once the sagittal ridge bone was exposed a high speed handpieve and burr was used to make an initial cross cut to determine the maximum depth of bone removal. From this depth cut line the ridge was reduced forward and backward to the extent of the external markings.
Once the sagittal ridge bone was exposed a high speed handpieve and burr was used to make an initial cross cut to determine the maximum depth of bone removal. From this depth cut line the ridge was reduced forward and backward to the extent of the external markings.
 After flushing out the pocket to remove any remaining bone particles closure was done with resorbable sutures over a drain.
After flushing out the pocket to remove any remaining bone particles closure was done with resorbable sutures over a drain.
 Sagittal ridge reduction is a successful procedure when the patient via the CT scan has confirmed that enough bone can be removed. It is thus a safe procedure whose recovery is very rapid from it. Even in a shaved head the incision heals very well and has never been an aesthetic distraction from the appearance of the reduced ridge.
Sagittal ridge reduction is a successful procedure when the patient via the CT scan has confirmed that enough bone can be removed. It is thus a safe procedure whose recovery is very rapid from it. Even in a shaved head the incision heals very well and has never been an aesthetic distraction from the appearance of the reduced ridge.
Key Points:
) A preoperative 2D CT scan is a good preoperative evaluation of the potential success of sagittal ridge skull reduction surgery.
2) The vertical lines seen in the CT scan is the irregularly coursing fibrous tissue of the sagittal suture line.
3) In a sagittal ridge of at least 8cms length the small pependicular incision should be placed at its midpoint so the full length can equally be reached for reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon