

 Background: The shape of the back of the skull is particularly prone to developing undesired changes in its shape. Flattening and asymmetries are the results of in utero and postnatal deformational forces which can prevent a rounded head shape. While one form of flatness of the back of head is known as brachycephaly due to congenital synostosis of the lambdoid sutures, more moderate amounts of overall flatness have intact suture lines in adults.
Background: The shape of the back of the skull is particularly prone to developing undesired changes in its shape. Flattening and asymmetries are the results of in utero and postnatal deformational forces which can prevent a rounded head shape. While one form of flatness of the back of head is known as brachycephaly due to congenital synostosis of the lambdoid sutures, more moderate amounts of overall flatness have intact suture lines in adults.
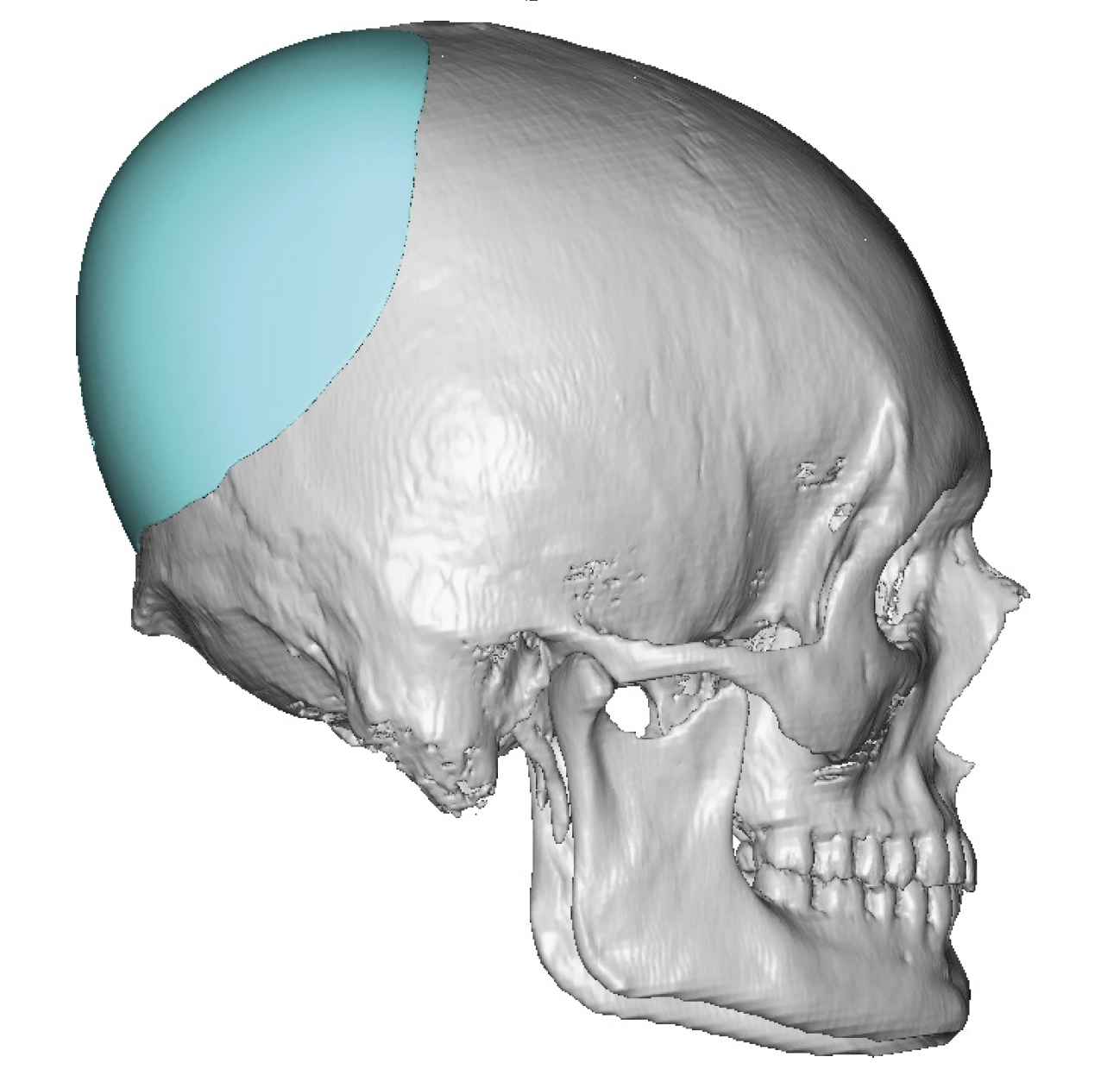
When correcting the shape of the back of the head the most effective method is a computer implant design. Getting a good shape , adequate projection and good symmetry between the two sides requires more surface area of implant coverage that one would think. While the back of the head has increased projection its perimeter footprint must cross over onto the top and sides of the skull. A 3D CT skull scan provides a full visual assessment of the scope of the deformity for all angles from which a good corrective design can be done.
When adding projection to the back of the head it is important to also realize that the scalp coverage is also diminished. Thus the amount of implant projection added will be controlled by the tension placed on the overlying scalp which must contain it. The scalp can only be safely stretch so much to avoid stress on the hair follicles and the blood flow to the central part of the area off maximal projection. This is not an exact science to determine what those limits are other than a lot of experience performing the procedure.
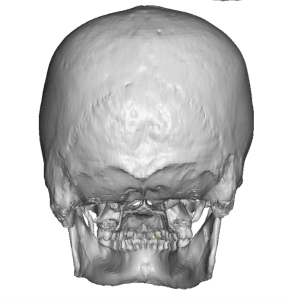
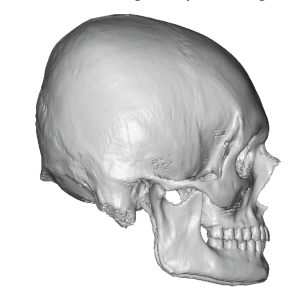 Case Study: This young male was bothered by the flatness of the back of the head which he kept hidden by his long hair. His 3D CT scan showed the lack of projection of the occipito-parietal skull with a compensatory increase in the crown of the skull.
Case Study: This young male was bothered by the flatness of the back of the head which he kept hidden by his long hair. His 3D CT scan showed the lack of projection of the occipito-parietal skull with a compensatory increase in the crown of the skull.
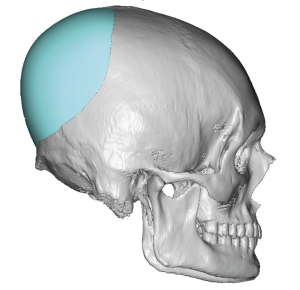 A custom skull implant was designed which added 14mm of implant projection with an implant volume of 100ccs. The volume number is more important than the maximum implant thickness as the scalp acts like a tent over the implant projection.
A custom skull implant was designed which added 14mm of implant projection with an implant volume of 100ccs. The volume number is more important than the maximum implant thickness as the scalp acts like a tent over the implant projection.

 Under general anesthesia and in the position a 7cm scalp incision was made over the nuchal ridge after creating a two ponytail part in the hair.. A large subperiosteal pocket was made into which the implant was placed and secured with micro screws. The scalp incision was closed with resorbable sutures over a drain.
Under general anesthesia and in the position a 7cm scalp incision was made over the nuchal ridge after creating a two ponytail part in the hair.. A large subperiosteal pocket was made into which the implant was placed and secured with micro screws. The scalp incision was closed with resorbable sutures over a drain.

 When seen the next day the improvement in the shape of the back of his head could be appreciated even with his long hair.
When seen the next day the improvement in the shape of the back of his head could be appreciated even with his long hair.
While some may think that long hair can adequately hide a skull shape deformity, and int certainly would seem rot do so looking externally, that often does not change the patient’s internal awareness of it. In fact the patient may not really prefer to wear their hair that way but does so because of their sensitivity to it. The surgery may allow them to wear a more desired shorter hairstyle.

 Long hair does not prevent skull implant augmentation surgery nor is there great benefit to shaving the hair to do so. The location of the incision can become clearly seen by carefully parting the hair and then placing it into two pulled back pony tails. Having the hair in the surgical field does not appear to increase the risk of postoperative infection based on my extensive experience.
Long hair does not prevent skull implant augmentation surgery nor is there great benefit to shaving the hair to do so. The location of the incision can become clearly seen by carefully parting the hair and then placing it into two pulled back pony tails. Having the hair in the surgical field does not appear to increase the risk of postoperative infection based on my extensive experience.
Key Points:
1) The flat back of the heed can be hidden by long hair as a compensatory method of camouflage.
2) It is not necessary to cut long hair for placing a custom back of the head skull implant.
3) The long hair helps in the recovery process both by camouflage of swelling and the incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon