


Background: The back of the head is unique in many ways but is the only skull surface that can have bone and scalp aesthetic deformities. The back of the head can have bony protrusions such as occipital knobs and buns as well as a wide variety of bony flattening and asymmetry shapes. Excess scalp can also appear as rolls at the junction of the bottom of the occipital skull bone and the neck muscles. Such scalp rolls appear in a variety of involvement from single to even triple scalp roll deformities.
Usually you see back of the head bone and scalp deformities as separate aesthetic issues but rarely they can appear together. When it is a skull deficiency that requires a custom implant augmentation the first question is what incisional approach is needed for its placement and can the scalp roll excision site be used for it. (presumably and ideally yes) Then the question becomes what type of scalp roll excision is needed.
Scalp rolls are redundant soft tissue that appears as horizontal rolls with a indentation lines above or below. Usually the deepest indentation line is on its underside directly again the lower end of the occipital bone. (aka nuchal ridge) This indicates that the excess scalp roll is ‘hanging over’ the end of the bone. When a single scalp roll is present its partial or complete excision with a horizontal scar tradeoff is an obvious surgical solution. But when double and triple scalp rolls or very deep indentation above and below a single roll exist the surgical solution is not so straightforward.
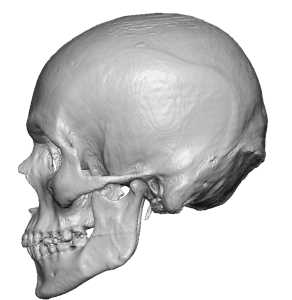
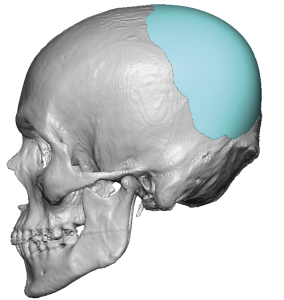 Case Study: This male had a back of the head flattening that he wanted improved using a custom skull implant. To provide an effective augmentation a custom skull implant was designed with a total volume of 80ccs.
Case Study: This male had a back of the head flattening that he wanted improved using a custom skull implant. To provide an effective augmentation a custom skull implant was designed with a total volume of 80ccs.
 He also mentioned that he had a ‘bone’ that stuck out from the back which was presumed to be an occipital knob based on a profile picture. But in seeing him in person it turned out to be a large scalp roll with deep indentation line above and below. The lower indentation line was stuck to the bone. The only method to improve such scalp rolls is excision of which the only question is whether it can partially or fully be cut out and how much scar length is aesthetically tolerable.
He also mentioned that he had a ‘bone’ that stuck out from the back which was presumed to be an occipital knob based on a profile picture. But in seeing him in person it turned out to be a large scalp roll with deep indentation line above and below. The lower indentation line was stuck to the bone. The only method to improve such scalp rolls is excision of which the only question is whether it can partially or fully be cut out and how much scar length is aesthetically tolerable.
 Under general anesthesia and in the prone position an initial incision was made in the deep horizontal indentation line under the scalp roll. Subperiosteal dissection was made up over the occipital bone but to do an adequate anterior dissection a small scalp incision in the crown area was added to ‘turn the corner’ well as serve as exposure of the orientation marker on the implant. (created by 4mm dermal punch holes)
Under general anesthesia and in the prone position an initial incision was made in the deep horizontal indentation line under the scalp roll. Subperiosteal dissection was made up over the occipital bone but to do an adequate anterior dissection a small scalp incision in the crown area was added to ‘turn the corner’ well as serve as exposure of the orientation marker on the implant. (created by 4mm dermal punch holes)
 The skull implant was inserted and positioned using the superior scalp incision with visualization of the implant marker. Once aligned and in good perceived position double screw fixation was applied.
The skull implant was inserted and positioned using the superior scalp incision with visualization of the implant marker. Once aligned and in good perceived position double screw fixation was applied.

 The scalp roll had been previously released and undermined as part of the implant pocket dissection. To keep the incisional scar limited to the length of the current indentation line, a subtotal scalp roll excisions was done. A complete excise was done centrally but had to taper down to the sides to avoid making a much longer scar. The scalp roll closure was then don e over a drain.
The scalp roll had been previously released and undermined as part of the implant pocket dissection. To keep the incisional scar limited to the length of the current indentation line, a subtotal scalp roll excisions was done. A complete excise was done centrally but had to taper down to the sides to avoid making a much longer scar. The scalp roll closure was then don e over a drain.

 When see the next day for head dressing and drain removal, the improvement in the back of his head was seen in profile.
When see the next day for head dressing and drain removal, the improvement in the back of his head was seen in profile.

 In the back view assessment the reduction in the scalp roll was seen but with a non-straight closure line.
In the back view assessment the reduction in the scalp roll was seen but with a non-straight closure line.
Highlights:
- Scalp rolls on the back of the head can camouflage as bone deformities in profile.
- Scalp roll excision can be done as part of a back of the head reshaping with a custom skull implant.
- The custom skull implant can be inserted through the scalp roll excision but may need a small dissection/placement incision to guide the implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon