


Background: Cheek augmentation is most commonly done in females. The traditional goal was to create an ‘apple cheek’ midface effect. This is defined as the part of the cheek that enlarges when smiling or laughing. This is anatomically over the main anterolateral projection of the cheekbone and has a rounded appearance. To no surprise this is the typical shape of standard cheek implants, an oblong or oval shape which is to be placed over the main body of the cheekbone.
While off-the-shelf implants have evolved from basic oval shapes over the years to provide more specific types of cheek augmentation, they are still just variants of anterolateral cheek augmentation. While this still works well for some patients, it does not suit everyone. This is true for men in general and for some females that seek a very specific type of cheek look.
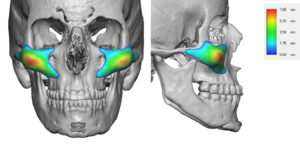
One type of specific midface effect that standard implants are not made for is the antero-inferior or malar-maxillary augmentation. This is for a forward type of cheek enhancement that places the point of maximal projection on the front end of the cheek bone beneath the eye. While one could use a standard implant and merely push it forward from its intended position on the cheek bone, it is important to appreciate the difference between the convex underside of the implant on a bone location that has a concave outer contour underneath it. This incompatibility of the implant’s and recipient’s bone contours has potential adverse issues.
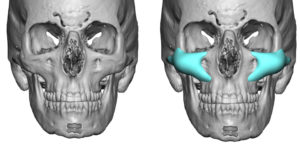
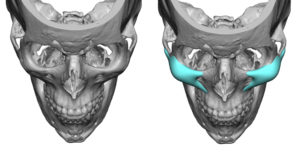
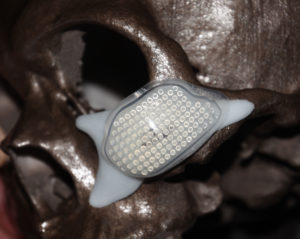
 Case Study: This young female sought a very specific type of cheek augmentation result. She wanted fullness anterior to the typical mid-cheek area. To do so a custom cheek implant design was done which used a more anatomically correct shape to the underlying bone with infraorbital-maxillary-arch extensions. This tripod design mimics that of the underlying zygomatic-maxillary bone shape. The point of maximal projection can then be aligned to whether the patient wants it but the implant’s base does not need to change.
Case Study: This young female sought a very specific type of cheek augmentation result. She wanted fullness anterior to the typical mid-cheek area. To do so a custom cheek implant design was done which used a more anatomically correct shape to the underlying bone with infraorbital-maxillary-arch extensions. This tripod design mimics that of the underlying zygomatic-maxillary bone shape. The point of maximal projection can then be aligned to whether the patient wants it but the implant’s base does not need to change.
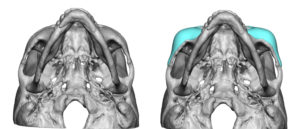
Under general anesthesia and through small intraoral vertical vestibular incisions, a wide subperiosteal pocket was made. The implant was positioned using the maxillary buttress extension as the point of alignment. Alignment is always important on cheek implants and is harder when it is just an oval shape with no defined reference points to its positioning. Fixation was achieved by a single screw placed into the thicker buttress bone.
 While standard cheek implant designs have a valuable role to play for many facial augmentation patients, more patients are seeking implants designed to their specific aesthetic needs. Using a tripod base concept the point of maximal projection can be moved around to best suit the patient’s aesthetic goals
While standard cheek implant designs have a valuable role to play for many facial augmentation patients, more patients are seeking implants designed to their specific aesthetic needs. Using a tripod base concept the point of maximal projection can be moved around to best suit the patient’s aesthetic goals
Case Highlights:
1) Cheek augmentation is best thought as where the patient wants the point of maximal projection/fullness.
2) The determination of the use of standard vs custom cheek implants is based on where that projection area is and by what amount does it need to be augmented.
3) An anterior malar cheek augmentation effect requires a custom design with an infraorbital and maxillary extensions.
Dr. Barry Eppley
Indianapolis, Indiana