

Background: The skull has five basic bony surfaces. The forehead, top and back of the head are exclusively bone surfaces while the paired side of the head is covered by a thick muscular layer. (temporalis muscle) This anatomic difference has great relevance when it comes to performing various skull augmentation procedures. While placing a skull implant on the forehead, top and back of head the placement is always on bone. Conversely augmentation on the side of the head must consider whether implant placement is submuscular (on the bone), subfascial (on top of muscle) or suprafascial. (on top of the deep temporal fascia)
In treating the narrow head shape distinction must be made between an incomplete or complete lack of adequate width. In the incomplete narrow head the main deficiency is central and is located above the ear. It can be treated by placing an implant under the muscle on top of the most convex part of the temporal bone. In the complete narrow head the width deficiency extends into the front and back skull surfaces as well. The forehead is a bit narrow on the sides as well as the same on the back of the head. Augmenting this type of narrow head can not be done by submuscular placement. Rather, because of the fascial attachments along the bony temporal line, an implant augmentation must be placed on top of the deep temporal fascia in order to cross onto the bone on the front and back of the head.
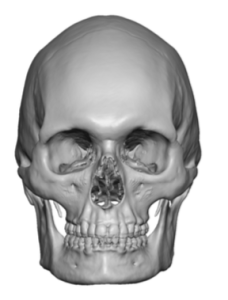
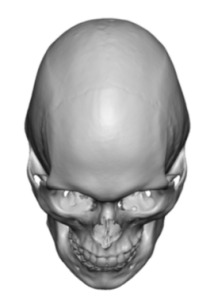
 Case Study: This male had a prior history of a successful skull augmentation on the upper back of the head as well as on top along the parasagittal bone surfaces. His original 3D CT scan prior to any implant placement showed the original shape of his skull.
Case Study: This male had a prior history of a successful skull augmentation on the upper back of the head as well as on top along the parasagittal bone surfaces. His original 3D CT scan prior to any implant placement showed the original shape of his skull.
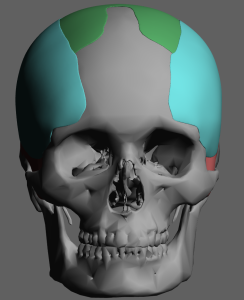
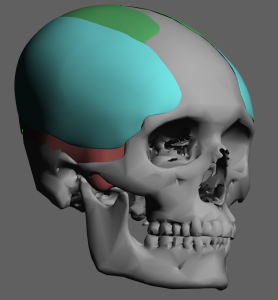
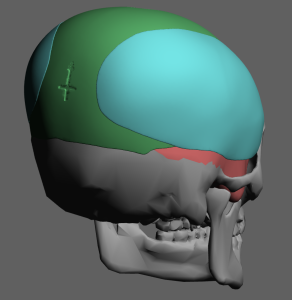
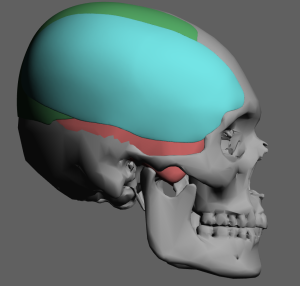 A custom temporal-forehead (complete head widening) implant was designed (teal color) that partially overlaid onto the prior skull implant on the top of the head. (green color) The second skull implant worked with the first one to fully correct the narrow head shape.
A custom temporal-forehead (complete head widening) implant was designed (teal color) that partially overlaid onto the prior skull implant on the top of the head. (green color) The second skull implant worked with the first one to fully correct the narrow head shape.
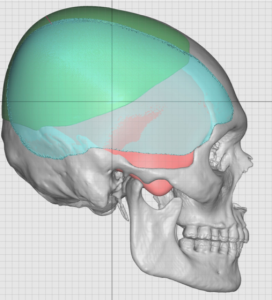 The extent of the integration/overlay of the two skull implants could be appreciated in the side view ‘see through’ design images.
The extent of the integration/overlay of the two skull implants could be appreciated in the side view ‘see through’ design images.
 Under general anesthesia postauricular incisions were made through blunt dissection on top of the deep temporal fascia was done to develop the implant pocket. The bony forehead part of the implant pocket was developed by a secondary small scalp incision just behind the frontal hairline on each side. Through his incision an elevator was used to make the angled transition between the bony forehead and the deep temporal fascia across the bony temporal line.
Under general anesthesia postauricular incisions were made through blunt dissection on top of the deep temporal fascia was done to develop the implant pocket. The bony forehead part of the implant pocket was developed by a secondary small scalp incision just behind the frontal hairline on each side. Through his incision an elevator was used to make the angled transition between the bony forehead and the deep temporal fascia across the bony temporal line.
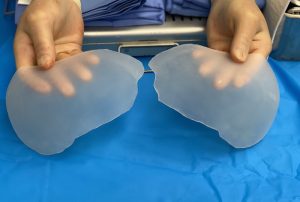
 The implants were rolled and inserted through the postauricular incisions. Once inside the pocket the implants were unrolled into its flat shape and then positioned as per the design. The most critical part of the positioning was on the forehead where good placement was needed to avoid postoperative visible implant edging.
The implants were rolled and inserted through the postauricular incisions. Once inside the pocket the implants were unrolled into its flat shape and then positioned as per the design. The most critical part of the positioning was on the forehead where good placement was needed to avoid postoperative visible implant edging.

 Fixation of the implants were done by single screw fixation at the frontal scalp incision as well as suture fixation at the implant edge seen through the postauricular incisions.
Fixation of the implants were done by single screw fixation at the frontal scalp incision as well as suture fixation at the implant edge seen through the postauricular incisions.

 The immediate before and after effects of the implants could be seen when viewed on the operative table.
The immediate before and after effects of the implants could be seen when viewed on the operative table.
Remarkably such a large head widening implant can be placed through a hidden postauricular and single small scalp incisions. The key to its placement is that it has to be on top of the deep temporal fascia to cross over onto the front and back of the bony skull surfaces. It illustrates that the side of the head is more soft tissue than bone and should be so augmented.
Case Highlights:
1) The narrow head is associated with temporal width deficiencies that often extended into the side of the forehead as well as the side of the back of the head.
2) An extended custom temporal implant can be designed and placed that wraps around the side of the head adding desired width.
3) This extended side of the head implant can be placed through a postauricualr incision behind the ear with one or two smaller positioning scalp incisions.
Dr. Barry Eppley
Indianapolis, Indiana