

Background: The face is prone to a wide variety of developmental abnormalities due to the paired nature of its embryologic development. A frequent cause of facial asymmetries comes from lower jaw development. Originating from the paired first pharyngeal or brachial arches, which develop as early as the fourth week of embryonic life, their eventual growth and midline merger in utero determines the final arch shape of the lower jaw. Should there be any difference in the growth between the two sides jaw/lower facial asymmetry will result.
While it is possible that one side of the lower jaw during development could over develop this is far more rare than that of lower jaw underdevelopment. While the most severe form of developmental lower jaw asymmetry is seen in the craniofacial syndrome of hemifacial microsoma, which occurs in about 1 in every 3,500 births, non-syndromic jaw asymmetry is far more common. Such aesthetic jaw asymmetries can be as slight as an inferior border difference between the two sides with a normal midline chin position to more profound asymmetries with chin deviation to the shorter side and a significant to the occlusal plane. Above the lower jaw asymmetry the facial features becomes less asymmetric and may or may not involved the cheek and orbits.
In lower facial asymmetries that involve an occlusal plane asymmetry, double jaw surgery is the standard and effective approach to level out the occlusal plane and straighten the face. Should this procedure not be desirable option the alternative approach is to camouflage the skeletal asymmetry with a custom jawline implant. The debate with a jawline augmentation approach is whether only the smaller jawline side should be build out or whether both sides of the jaw should be done. That would depend on how whether one is happy with the unaffected normal side of the lower jaw.
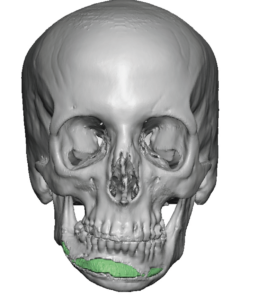
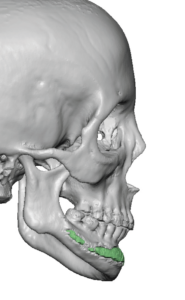 Case Study: This female had a significant lower jaw asymmetry with a right jawline in which the jaw angle was 10mms vertically shorter than the left side. This caused obvious chin asymmetry and a tilted occlusal plane. She also had a slightly smaller right cheekbone above it. She had never wanted to undergo double jaw surgery for her facial asymmetry correction. A chin implant had been previously placed but its high and tilted positioning did nothing to improve her asymmetry.
Case Study: This female had a significant lower jaw asymmetry with a right jawline in which the jaw angle was 10mms vertically shorter than the left side. This caused obvious chin asymmetry and a tilted occlusal plane. She also had a slightly smaller right cheekbone above it. She had never wanted to undergo double jaw surgery for her facial asymmetry correction. A chin implant had been previously placed but its high and tilted positioning did nothing to improve her asymmetry.
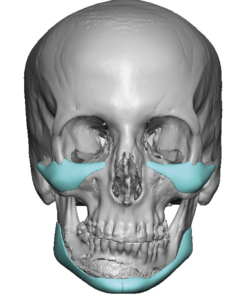
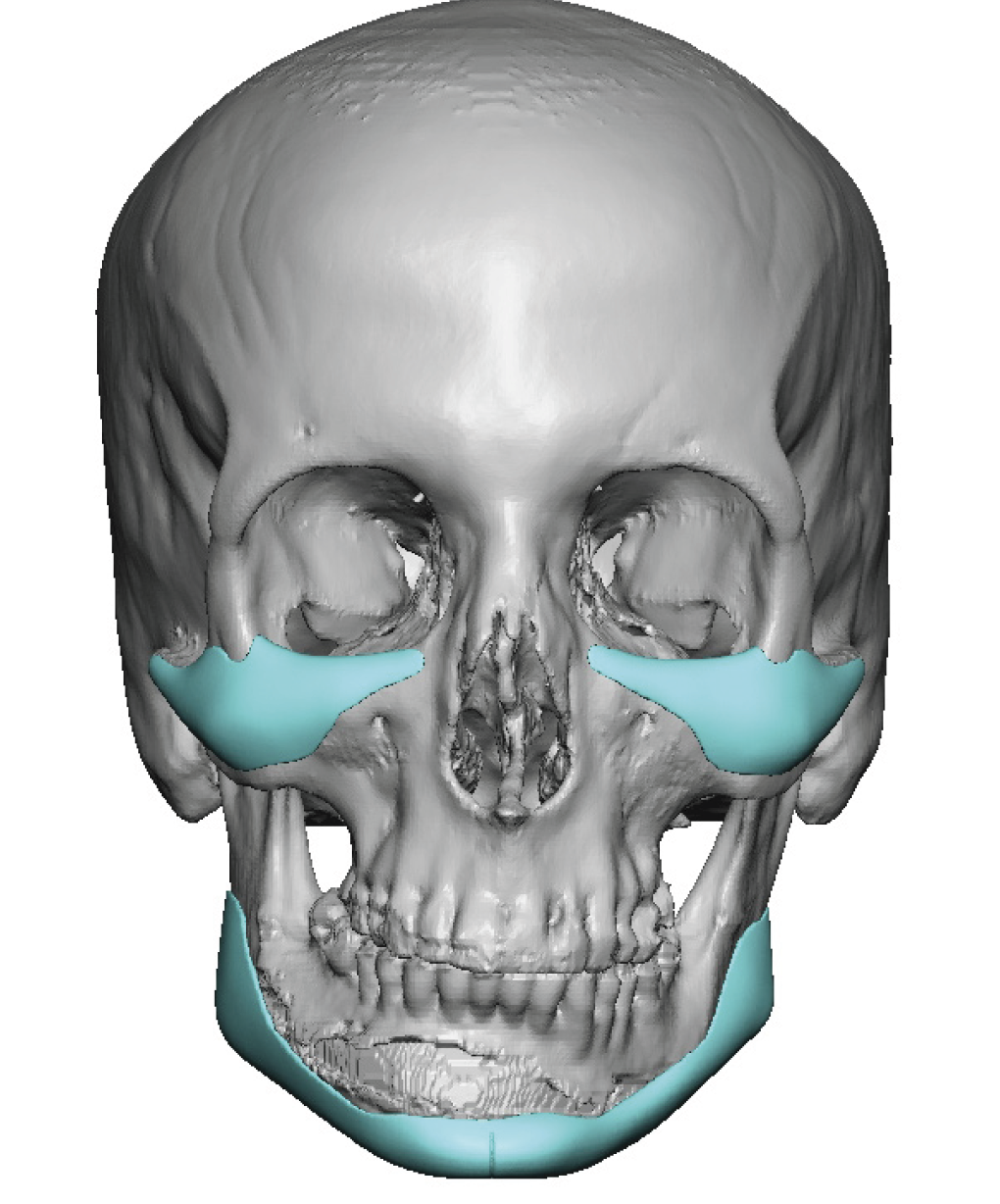
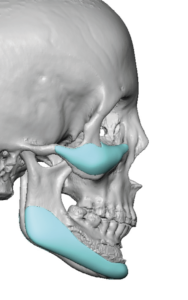 Custom infraornital-malar (for undereye hollows and cheek asymmetry correction) and a wrap around jawline implant were designed.
Custom infraornital-malar (for undereye hollows and cheek asymmetry correction) and a wrap around jawline implant were designed.
 She had all three custom facial implants placed and she went on to heal uneventfully without infection or impaired jaw function.
She had all three custom facial implants placed and she went on to heal uneventfully without infection or impaired jaw function.



 When seen at four months postop her jaw and lower facial asymmetry were much improved. Perfect symmetry is rarely achieved and there remains some telltale signs of the asymmetry such as the can’t of the mouth corners.
When seen at four months postop her jaw and lower facial asymmetry were much improved. Perfect symmetry is rarely achieved and there remains some telltale signs of the asymmetry such as the can’t of the mouth corners.
Case Highlights:
1) The lower face is often affected by asymmetric development which typically is seen in the bony lower jaw.
2) In an inferior or lower facial-based asymmetry the lower jaw is the most severely affected and the facial structures above it less so.
3) A custom jawline implant design is the most effective non-orthognathic surgery for lower jaw asymmetries.
Dr. Barry Eppley
World-Renowned Plastic Surgeon