

Background: Of all the standard facial implants that are available none is harder to properly position than the jaw angle implant. This is due to three reasons; 1) the working end of the jaw angle implant can not be seen from the intraoral incision, 2) the implant placement is in the most posterior part of the jaw where adequate subperiosteal pocket dissection requires a good understanding of the bony and muscular anatomy of the jaw angles and 3) it is a paired aesthetic structure which induces its own risks of asymmetric implant placement. As a result it is not quite as simple as making a pocket and simply sliding an implant into it.
Having performed other types of jaw angle surgeries such as sagittal split osteotomies and jaw angle fracture repairs is helpful, and actually technically more challenging, they differ in ways that are uniquely different from jaw angle implant placement. The sagittal split osteotomy is performed at the front region of the jaw angles where the bone cuts are largely performed under direct vision. Jaw angle fractures are often done through skin incisional approaches where the fracture alignment is clearly seen. And even if done intraorally the complete fracture line does not need to fully visualized to achieve a good repair.
Whether highly experienced or not the most common reason for jaw angle placement is inadequate posterior pocket development. The most common reason is that the ligamentous attachments and the posterior muscle border is not elevated resulting in an anterior location of the implant. This pushed the widening implant too far forward not putting the angle augmentation in the right location. With a vertically lengthening implant an undesired widening effect is created with no vertical increase at all.

 But one of most significant placement errors is when the anterior border of the jaw angle region is thought to be the posterior border. This may the partly explainable as plain x-rays make it appear that the jaw angles have a flat surface…when in fact they have a concavity (muscle fossa) between the raised anterior and posterior bony borders which is most pronounced in males. This can only be appreciated by anatomic dissections or the study of 3D CT scans.
But one of most significant placement errors is when the anterior border of the jaw angle region is thought to be the posterior border. This may the partly explainable as plain x-rays make it appear that the jaw angles have a flat surface…when in fact they have a concavity (muscle fossa) between the raised anterior and posterior bony borders which is most pronounced in males. This can only be appreciated by anatomic dissections or the study of 3D CT scans.
 Case Study: This male had widening jaw angle implants which results in immediate cheek swelling but no swelling over the jaw angles. The patient was certain there was something wrong with the implant placements but was assured they were in good position. As the swelling subsided it became apparent that the jaw angle implants were not in the correct location on the bone. A 3D CT confirmed the patient’s suspicion as the implants never made it much past the front region of the ramus.
Case Study: This male had widening jaw angle implants which results in immediate cheek swelling but no swelling over the jaw angles. The patient was certain there was something wrong with the implant placements but was assured they were in good position. As the swelling subsided it became apparent that the jaw angle implants were not in the correct location on the bone. A 3D CT confirmed the patient’s suspicion as the implants never made it much past the front region of the ramus.
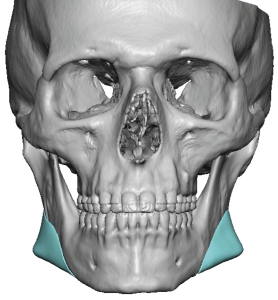
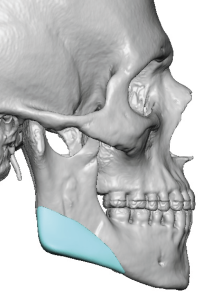
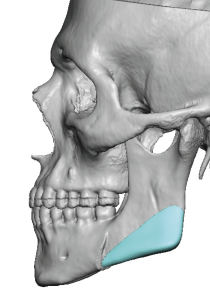
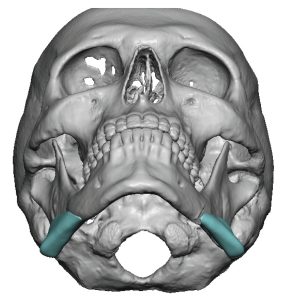 For his replacement surgery custom jaw angle implants were designed for a specific widening effect directly over the posterior-inferior angle area.
For his replacement surgery custom jaw angle implants were designed for a specific widening effect directly over the posterior-inferior angle area.
 Under general anesthesia and through his intraoral vestibular scars his indwelling jaw angle implant were removed as they were right under the mucosa over the ascending ramus. Comparing the removed implants with their replacement showed the difference but the implant placement was going to be more important than their shape and size.
Under general anesthesia and through his intraoral vestibular scars his indwelling jaw angle implant were removed as they were right under the mucosa over the ascending ramus. Comparing the removed implants with their replacement showed the difference but the implant placement was going to be more important than their shape and size.
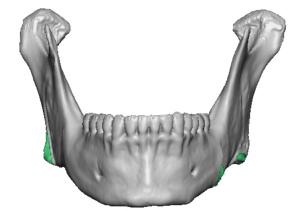
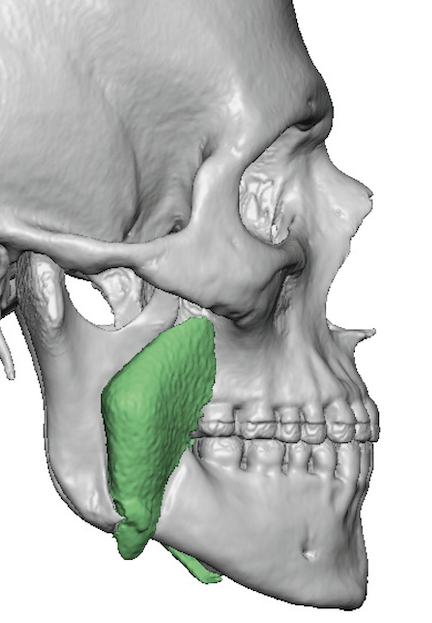
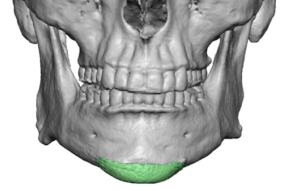
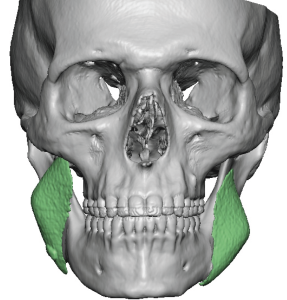
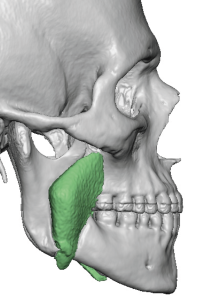
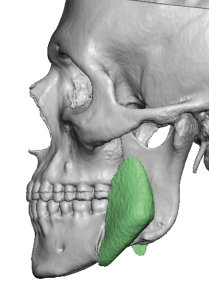
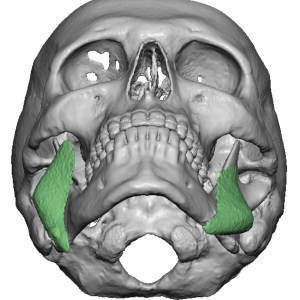
 To create an adequate pocket for the new implants the existing capsule on the bone needed to be completely removed. And of even greater importance is the need to remove the bony overgrowths around the removed implants. (in green color) Without these bone removals the new implants would not be able to placed properly.
To create an adequate pocket for the new implants the existing capsule on the bone needed to be completely removed. And of even greater importance is the need to remove the bony overgrowths around the removed implants. (in green color) Without these bone removals the new implants would not be able to placed properly.
This is a fairly severe case of jaw angle implant malpositioning that was so significant one wonders if they had ever done the procedure before. At the least the extent of intraoral dissection was woefully inadequate and it is clear that they did not appreciate where the posterior border of the ramus was located. They got fooled by not knowing that the bony jaw angle turns inward behind the last molar tooth which makes the posterior border very hard to see.
Key Points:
1) Jaw angle implant malpositions take on predictable patterns due a lack of anatomic understanding and inadequate pocket development as a result.
2) Intraoral visualization is inadequate to ensure that the jaw angle implant is in proper position over the genial angle.
3) Custom jaw angle implants may provide shape improvements over standard implants but they still have to be properly placed to get the full benefits of the design.
Dr. Barry Eppley
World-Renowned Plastic Surgeon