


Background: Jaw angle implants pose very difficult challenges than chin implants in both size and style selection as well as surgical placement. The most obvious difference is that a chin implant is a single procedure while jaw angle implants are two procedures due to their bilateral locations. Positioning a single implant over a solitary projecting chin bone has less risk of complications than trying to position two implants symmetrically over what are often asymmetric jaw angle shapes that covered by thick muscle tissue.
A less obvious difference is that the working end of a chin implant is in the direct line of vision from the incision regardless if it is intraoral or submental. Conversely the working end of the jaw angle implant can not be seen from the intraoral incision as it’s superior portion blocks visualization of the inferior and posterior working angle portion of the implant. Thus it is very diffcult to tell exactly where the jaw angle implant is on the bone. It is largely guided by a few surrounding bony landmarks and external palpation …a far cry of how a chin implant is placed.
As a result jaw angle implant asymmetry is really the norm and not the exception. Custom jaw angle implants fare better for the obvious reason that they are designed specifically for the patient’s jaw angle bony shape and there is intraoperative guidance for how the implant fits the bone from the design. That does not mean it is a guarantee for assured placements but the odds are better. But when custom jaw angle implants are used to replace undesired standard ones other variables in placement are encountered due to scarring and bony overgrowth.
 Case Study: This male has standard jaw angle implants placed but they did not produce his desired aesthetic effects and were also asymmetric. They were 10mm widening implants with the right in pretty good position but the left was anteriorly displaced. Of particular relevance was the large amount of superior bony overgrowth on each implant.
Case Study: This male has standard jaw angle implants placed but they did not produce his desired aesthetic effects and were also asymmetric. They were 10mm widening implants with the right in pretty good position but the left was anteriorly displaced. Of particular relevance was the large amount of superior bony overgrowth on each implant.
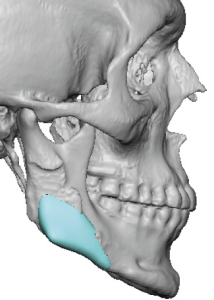
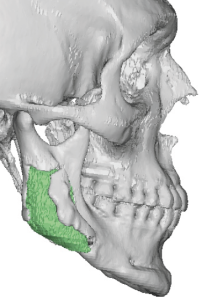
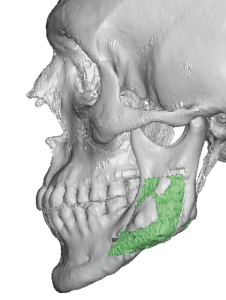
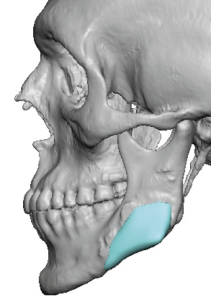 New custom jaw angle implants were designed of the same width but they were designer to be positioned anterior to the posterior border. The implant was positioned over the antegonial notch area, an uncommon location but one the patient felt had the best aesthetic look. (An observation learned from the anteriorly malpositoned left standard jaw angle implant)
New custom jaw angle implants were designed of the same width but they were designer to be positioned anterior to the posterior border. The implant was positioned over the antegonial notch area, an uncommon location but one the patient felt had the best aesthetic look. (An observation learned from the anteriorly malpositoned left standard jaw angle implant)

 Under general anesthesia and through his original intraoral posterior vestibular incisions the jaw angles were exposed showing initially the bony overgrowth. If one didn’t know there was an implant underneath it by a 3D CT scan it would be easy to assume there was no implant there.
Under general anesthesia and through his original intraoral posterior vestibular incisions the jaw angles were exposed showing initially the bony overgrowth. If one didn’t know there was an implant underneath it by a 3D CT scan it would be easy to assume there was no implant there.

 The bony ovegrowths, implants and fixation screws were removed and compared to the custom implant replacements. It is important to appreciate how much smaller the new custom implants were as they were to be placed into a much larger dissected pocket.
The bony ovegrowths, implants and fixation screws were removed and compared to the custom implant replacements. It is important to appreciate how much smaller the new custom implants were as they were to be placed into a much larger dissected pocket.
 Due to the original malposition of the left jaw angle implant pocket the new left custom implant fit right into it as designed. On the right side the original implant was more posterior to the desired location than where the new implant was to be positioned. Without specific anatomic landmarks the positioning of the new custom implant was estimated and placed anterior to the original implant location.
Due to the original malposition of the left jaw angle implant pocket the new left custom implant fit right into it as designed. On the right side the original implant was more posterior to the desired location than where the new implant was to be positioned. Without specific anatomic landmarks the positioning of the new custom implant was estimated and placed anterior to the original implant location.
Jaw angle implants commonly develop bony overgrowths on their superior surface. This is due to the elevation of the periosteum over the muscle and is a form of reparative response to the implant. I have seen it many times both on 3D CT scans as well as in jaw angle implant revisions. If the surgeon is not aware that such bone overgrowths are present it would be easy to assume that there was no implant there. The bone overgrowth can be removed by osteotomes to expose the implant for removal.
But the hardest party of jaw angle implant replacements is their positioning on the bone. Where to place them exactly defies a precise method to do so given the limited visibility from the intraoral incision. In this case the left jaw angle implant was guided by the established pocket positioning. On the right side however the new implant position had to be guided more by knowing that it was anterior to the previous implant location.
Case Highlights:
1) Jaw angle implants are the most challenging of all facial implants to successfully place and get the desired effect.
2) If primary placement of jaw angle implants is difficult revisions of them are even more so due to scar tissue and bone overgrowth that occurs around them..
3) There are few registration landmarks in the jaw angle area to help guide placement, particularly when placed in a non-traditional location.
Dr. Barry Eppley
World-Renowned Plastic Surgeon