

Background: Reductive shoulder reshaping, often called shoulder narrowing surgery, works by shortening the length of the clavicles. Through a small incision located in the supraclavicular fossa a segment of the clavicle is removed and the ends reapproximated. This pulls in the distal clavicle and shoulder because the medial end of the clavicle, its sternoclavicular joint and the sternum are fixed structures. How much the shoulder moves inward depends on the length of the bone segment removed.
When removing the bone segment the approach to date has been to pick a fixed length, usually 2.5cms, to be removed on each side. While there is nothing wrong with this approach based on patient outcomes and satisfaction, it is necessary to slide the incision around to get the proximal and distal access for the bone removal. This often traumatizes the skin edges from the retraction more than I would like and could adversely affect how the scar heals…small as it is. An alternative technique is the telescoping osteotomy method described below.
Shoulders are well known to have asymmetry as their lengths are not perfectly equal.Most of the time this asymmetry is measurable but not always that visible. When such asymmetry occurs it is more commonly seen on the left side. When the shoulder asymmetry is clearly visible the bone length discrepancy could easily be 5 to 7mms and in some cases as much as 1 cm. With this increased length the curvature is often stronger or more exaggerated. This increased curvature may affect the shape of the shoulder when greater lengths are removed to try and improve symmetry.
 Case Study: This young female desired to have her shoulders narrowed with a buldeltoid distance of 46cms. She had a noticeable shoulder asymmetry with the left shoulder being wider with a longer and more curved clavicle shape.
Case Study: This young female desired to have her shoulders narrowed with a buldeltoid distance of 46cms. She had a noticeable shoulder asymmetry with the left shoulder being wider with a longer and more curved clavicle shape.
 Under general anesthesia and in the supin
Under general anesthesia and in the supin

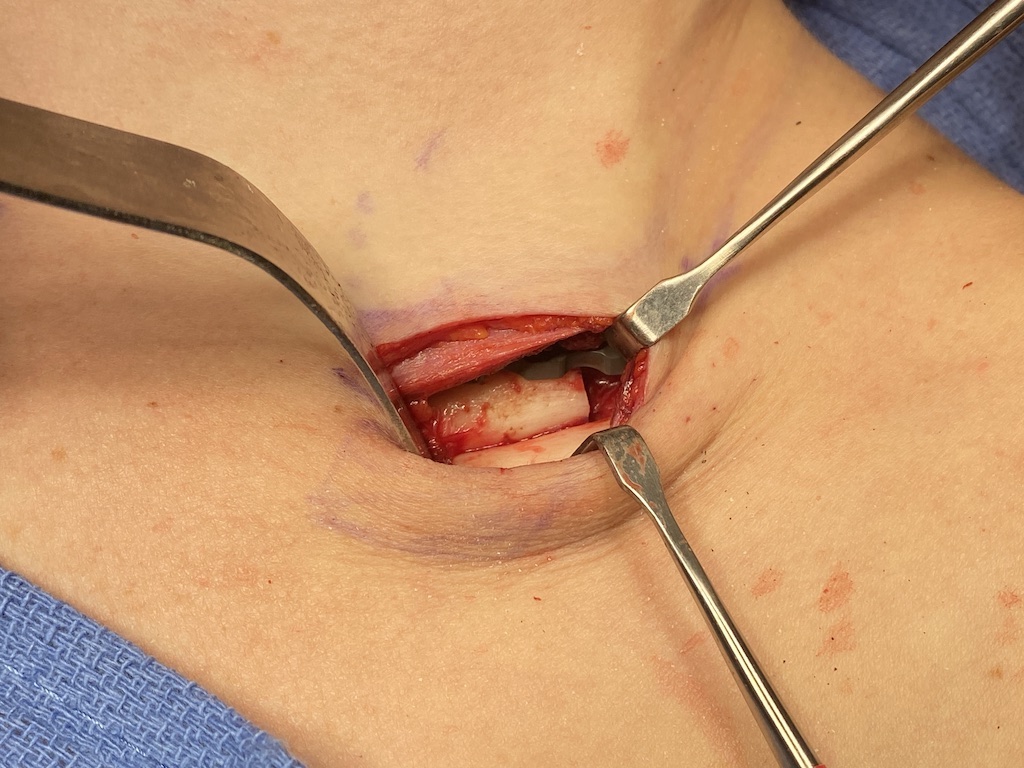
e position 4cm supraclavicukar fossa incisions were made and the clavicles circumferentially dissected out. The medial bone cut was made which allowed the distal end of the bone to collapse (telescope) past the cut proximal bone. The distal end of the bone was pulled out of the incision and a 3cm length length removed on the left side and 2.25cs on the right.
 The bone ends were put together with a superior 3.5mm and an anterior 2.5 mm plate and screws.
The bone ends were put together with a superior 3.5mm and an anterior 2.5 mm plate and screws.

 Her immediate before and after showed the change in her shoulder shape.
Her immediate before and after showed the change in her shoulder shape.
Asymmetry in shoulder width/shape is not usually treated by differential bone excisions unless it is a significant aesthetic issue for the patient. Shoulder asymmetry is common and such differences are usually less than 1 cm between the two sides. More pertinently any attempt at differential bone length excisions will be in the 5 to 7mm range as the smaller side has to be reduced at least by 2 mms if not more.
The telescoping technique is a technical change to removing the clavicle bone segment. Besides helping with incisional length it also allows both ends of the cut clavicle bone to better match in their angulations since the distal cut is now laying parallel to the proximal bone cut.
Case Highlights:
1) Shoulder length asymmetry is not uncommon, often with the left being the longer/larger side. In shoulder narrowing surgery the longer side can have moire bone taken to both reduce its length as well as improve shoulder symmetry.
2) The telescoping method of clavicle bone removal allows for a more measured method of removal while keeping the incision length limited.
3) Double plate and screw fixation is still applied for maximal bone stability of the reaproximated bone segments.
Dr. Barry Eppley
World-Renowned Plastic Surgeon