

Background: The historic approach to complete jawline augmentation is with the use of standard styles and sizes of chin and jaw angle implants. This three implant approach can be effective but is prone to asymmetries of implant positioning, an incomplete jawline effect and limitations of shapes and sizes of implants that are commercially available.
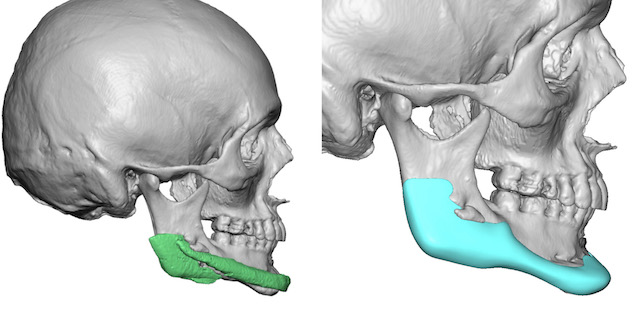
The one-piece custom implant approach has proven to be superior to the use of standard implants for total jawline augmentation. Creating the desired implant dimensions that are specific for each patient as well as having an implant made to fit the patient’s bone surface has obvious advantages. A one-piece implant, while technically more challenging to place, also has a lower risk of asymmetry than three separate implants.
In my experience roughly 40% of patients that present for a custom jawline implant have existing chin, jaw angle or both chin and jaw angle implants in place. Implant asymmetries, incomplete jawline augmentation or less that desired aesthetic results are the reasons patients seek to improve their prior jawline implant results.

 Case Study: This young male presented with a horizontally ad vertically short lower jaw. He opted for a non-custom implant approach to his jawline augmentation which consisted of a sliding genioplasty for horizontal and vertical lengthening, standard vertical lengthening jaw angle implants, and a extended chin implant overlay that had been designed with long posterior wings that would overlap the jaw angle implants. His result from this procedure were actually quite good and he lived with the outcome for five years. Over time he developed some chronic soreness of the right jaw angle area which was presumed to be where the wings of the chin implant laid on the jaw angle implant.
Case Study: This young male presented with a horizontally ad vertically short lower jaw. He opted for a non-custom implant approach to his jawline augmentation which consisted of a sliding genioplasty for horizontal and vertical lengthening, standard vertical lengthening jaw angle implants, and a extended chin implant overlay that had been designed with long posterior wings that would overlap the jaw angle implants. His result from this procedure were actually quite good and he lived with the outcome for five years. Over time he developed some chronic soreness of the right jaw angle area which was presumed to be where the wings of the chin implant laid on the jaw angle implant.
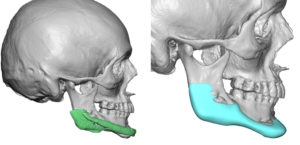
 As a result he opted to replace his existing implants with a custom jawline implant that replicated most of his existing implant dimensions with the exception of some additional jaw angle implant widths.
As a result he opted to replace his existing implants with a custom jawline implant that replicated most of his existing implant dimensions with the exception of some additional jaw angle implant widths.

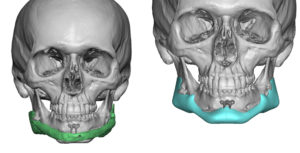
 Under general anesthesia his existing submental and intraoral incisions were used to remove his existing implants and replace them with the custom jawline implant. Given the tight capsular tissue underneath the mental nerve the jawline implant was placed through a geometric midline split technique in a back to front insertion method. The two sides of the chin was brought together in the midline and secured with screws. The jaw angle portions were secured with screws placed from an intraoral approach.
Under general anesthesia his existing submental and intraoral incisions were used to remove his existing implants and replace them with the custom jawline implant. Given the tight capsular tissue underneath the mental nerve the jawline implant was placed through a geometric midline split technique in a back to front insertion method. The two sides of the chin was brought together in the midline and secured with screws. The jaw angle portions were secured with screws placed from an intraoral approach.
One advantage of indwelling standard implants is that they provide dimensional guidance as to how design a custom implant. Most of the time patients opt for more significant dimensions in their new implant. This case is exceptional in that there was implant discomfort as the motivating factor and not an aesthetic dissatisfaction. Presumably having two overlapping implants may be the source of the discomfort of which a one piece replacement would resolve.
Case Highlights:
1) Standard chin and jaw angle implants can be an effective approach to total jawline augmentation but can have problems with asymmetry or implant displacement.
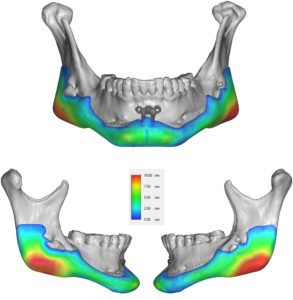
2) The existing implants provide a good dimensional guide to designing a one-piece custom jawline implant replacement.
3) The tight capsular lining of the existing implant pockets may make it necessary to use a split implant insertion technique.
Dr. Barry Eppley
Indianapolis, Indiana