

Background: While chin implants are commonly performed and many plastic surgeons perform them that does not mean that all results are similar. While an implant provides an assured volume effect, it still requires being properly positioned on the bone. This takes into account not only symmetry but placement on the bone where its effect can be maximally shown.
While these tenets of chin implant placement sound intuitive and easy they can become confounded by the incisions needed to place them. Whether such incisions are under the chin or intraoral, the size of the incisions used are always smaller than the implant itself. This translates into an operation which involves a portion of which is not seen. The full extent of the tissue pocket on the bone and the sides of the implant are not seen. This makes chin implant placement very different than just sticking it on a skeletal model.
As a result chin implant malpositions are not rare, and by 3D CT scan assessments of implant placements, are actually common. Whether the implant malpositioning affects the external aesthetic result depends on the type and extent. One of the most common chin implant malpositions is vertical. High and low positions are both seen some of which is created by failure to recognize where the implant should be placed for optimal effect. (or to avoid an adverse effect) Implants that after placed too high result in loss of some of the augmentation effect due to the inward incline of the chin bone.
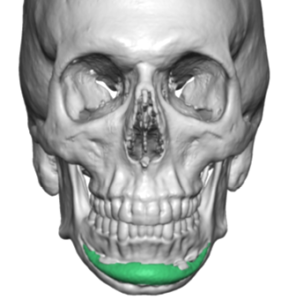
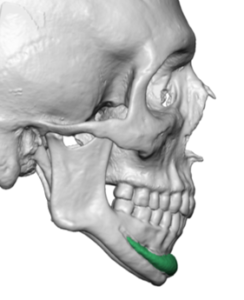 Case Study: This male had a prior extended chin implant placed which did not produce as much chin augmentation effect as he desired. He decided rather than get a new chin implant that he would get a total jawline implant instead. The 3D CT scan needed for the jawline implant design showed a highly positioned chin implant…but it was symmetrically positioned.
Case Study: This male had a prior extended chin implant placed which did not produce as much chin augmentation effect as he desired. He decided rather than get a new chin implant that he would get a total jawline implant instead. The 3D CT scan needed for the jawline implant design showed a highly positioned chin implant…but it was symmetrically positioned.
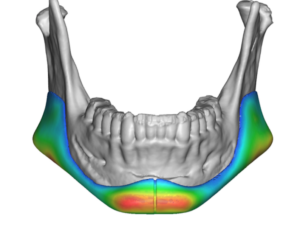
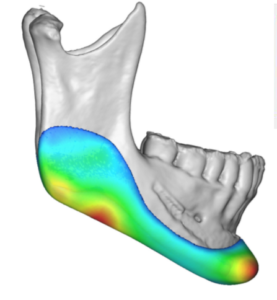
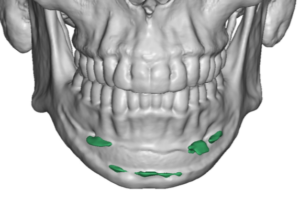 Digitally removing the chin implant showed the imprint of the implant on the bone and the locations of areas of bony overgrowths. (green color)
Digitally removing the chin implant showed the imprint of the implant on the bone and the locations of areas of bony overgrowths. (green color)
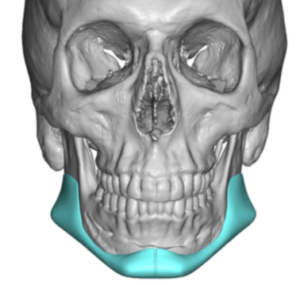
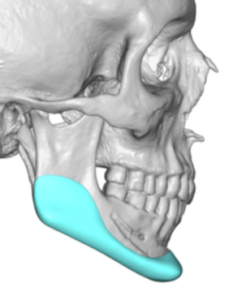
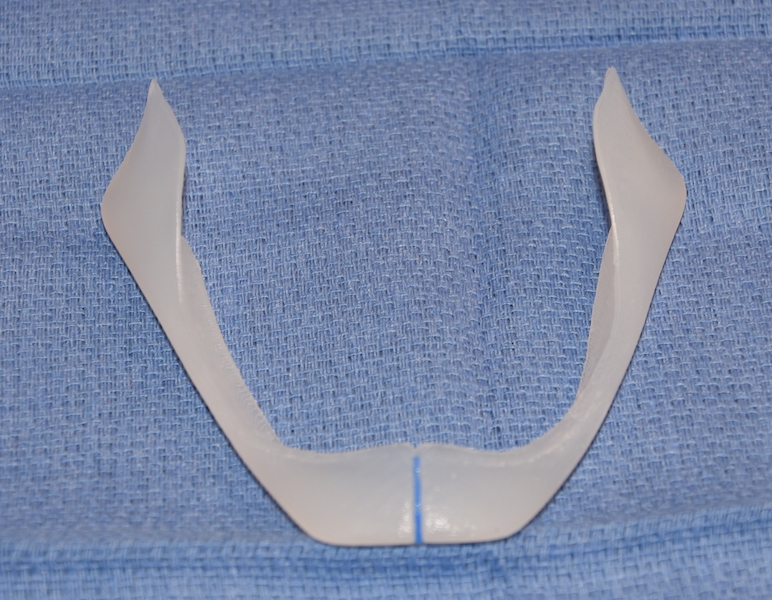
 A custom jawline implant was designed from his 3D CT scan that had a focus an enhancement but not or a major or very strange jawline augmentation change. The implant’s total volume was 16ccs.
A custom jawline implant was designed from his 3D CT scan that had a focus an enhancement but not or a major or very strange jawline augmentation change. The implant’s total volume was 16ccs.

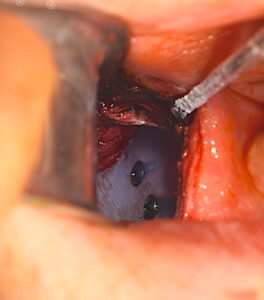 Through his existing submental scar, the indwelling chin implant was explanted, the bony overgrowths removed by osteotomes, inferior capsulotomies performed and the pocket extended back towards the jaw angles. The jaw angle pockets were made by posterior vestibular incisions. The jawline implant was then placed in a front to back insertion technique as a one piece implant. Screws were applied at the three corners.
Through his existing submental scar, the indwelling chin implant was explanted, the bony overgrowths removed by osteotomes, inferior capsulotomies performed and the pocket extended back towards the jaw angles. The jaw angle pockets were made by posterior vestibular incisions. The jawline implant was then placed in a front to back insertion technique as a one piece implant. Screws were applied at the three corners.
 The aesthetic migration from a chin implant to a total jawline implant is often a natural progression. It occurs due to either an unsatisfactory chin implant result or the appreciation that a satisfactory chin implant result is incomplete. In either case it is important for the surgeon to recognize that the indwelling chin implant is associated with a thick capsule and often bony overgrowths. Knowing where they are located by a 3D CT scan enables them to be reduced/removed so as to not interfere placement with the new implant.
The aesthetic migration from a chin implant to a total jawline implant is often a natural progression. It occurs due to either an unsatisfactory chin implant result or the appreciation that a satisfactory chin implant result is incomplete. In either case it is important for the surgeon to recognize that the indwelling chin implant is associated with a thick capsule and often bony overgrowths. Knowing where they are located by a 3D CT scan enables them to be reduced/removed so as to not interfere placement with the new implant.
Case Highlights:
1) Unsatisfactory chin implant results often become the nidus for upgrading to a total jawline augmentation.
2) Removal of the existing chin implant often involves capsulectomies/capsulotomies and the need for removal of areas of bony overgrowths.
3) Because the jawline implant by design augments the inferolateral border of the lower jaw, the full effect of the implant is always seen.
Dr. Barry Eppley
Indianapolis, Indiana