

Background: The anatomy of the jaw angle area is unique when it comes to implant augmentation. It is the only facial area where strong insertion ligamentous attachments need to be released for proper implant positioning. While this is an absolute technical requirement in implants that lengthen this part of the jaw it is still needed to a lesser degree when only jaw angle width enhancement is desired.
While release of the ligamentous attachments are a necessary part of the jaw angle procedure care must be taken in doing so. While the masseter muscle does not actually wrap around the inferior border of the jaw and attach directly to the pterygoid muscle on the other side it does have a periosteal attachment at the inferior border. This must be carefully elevated and preserved so the muscle does not retract up over the implant after surgery. (masseter muscle dehiscence)
While careful masseter muscle sling dissection must always be done to prevent detachment and retraction it can not always be avoided. There are patients who are at higher risk for such muscle dehiscence as I have learned from looking at thousands of 3D CT scans in jaw augmentation surgery. The shape of the jaw, size of the masseter muscles and gender all influence how strong the ligamentous attachments are and how successfully they can be elevated without a significant risk of postop muscle dehiscence.
In the instance where very strong ligamentous attachments exist and only width is needed for the desired jaw angle augmentation the custom jawline implant can be designed around them. This would reduce the potential risk of masseteric muscle dehiscence to zero.
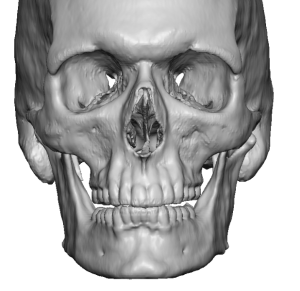
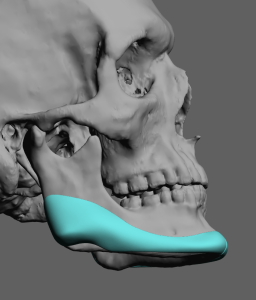
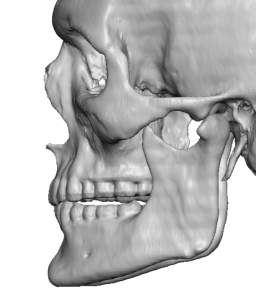 Case Study: This young male desired a custom jawline implant with primary emphasis on jaw angle width increase. His 3D Ct scan showed a flat mandibular plane angle, square shaped ramus and large spikes of bone along the inferior border of the angle.
Case Study: This young male desired a custom jawline implant with primary emphasis on jaw angle width increase. His 3D Ct scan showed a flat mandibular plane angle, square shaped ramus and large spikes of bone along the inferior border of the angle.
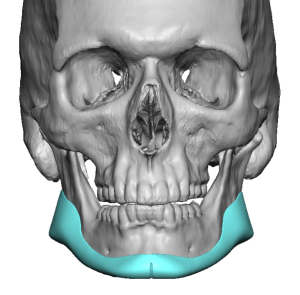
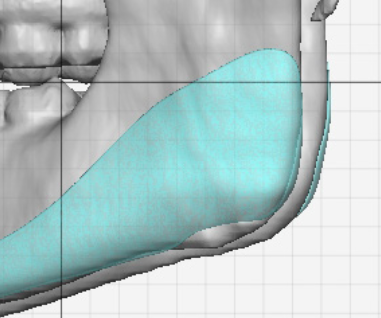
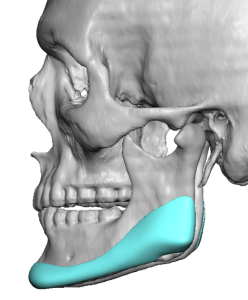 His custom jawline implant design had minimal chin projection, followed the shape of his natural jawline and added 12mms of jaw angle width but left a material void over the bony spikes of the jaw angles. (ligamentous attachments)
His custom jawline implant design had minimal chin projection, followed the shape of his natural jawline and added 12mms of jaw angle width but left a material void over the bony spikes of the jaw angles. (ligamentous attachments)
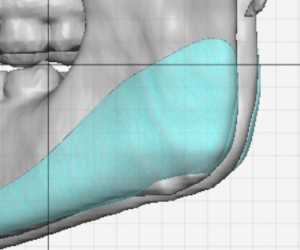
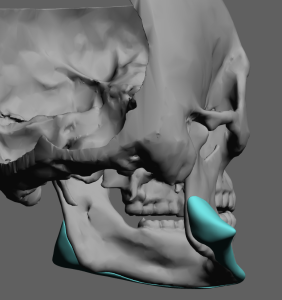
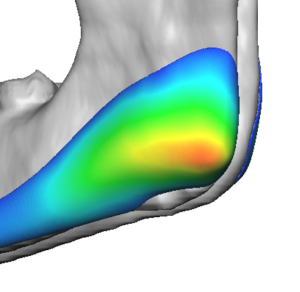 Close up evaluation of the implant design showed the ligamentous relief over and around them.
Close up evaluation of the implant design showed the ligamentous relief over and around them.
 Under general anesthesia and through the usual three incision approach the jawline implant was placed having the jaw angle sections sit on top of the ligamentous attachments. Before placement the reliefs could be seen on the inside of the implant.
Under general anesthesia and through the usual three incision approach the jawline implant was placed having the jaw angle sections sit on top of the ligamentous attachments. Before placement the reliefs could be seen on the inside of the implant.


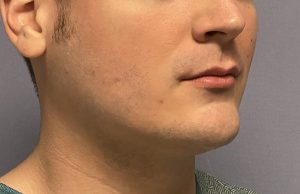
 When seen six months later the results of the custom jawline implant could be seen with no evidence of masseteric muscle dehiscence.
When seen six months later the results of the custom jawline implant could be seen with no evidence of masseteric muscle dehiscence.
 While it is ideal to have a jaw angle implant sit down along the inferior border to optimize its width effect one has to be mindful about the Masseter muscle ligamentous attachments. When they appear as profound spikes of bone, whether in one, two or three bony prominences per side, this indicates they will be very adherent and not easy to elevate off from the bone. Thus the risk of muscle dehiscence is increased. This risk can be negated, provide that only jaw angle width is needed, by making the implant design around them and leaving them intact.
While it is ideal to have a jaw angle implant sit down along the inferior border to optimize its width effect one has to be mindful about the Masseter muscle ligamentous attachments. When they appear as profound spikes of bone, whether in one, two or three bony prominences per side, this indicates they will be very adherent and not easy to elevate off from the bone. Thus the risk of muscle dehiscence is increased. This risk can be negated, provide that only jaw angle width is needed, by making the implant design around them and leaving them intact.
Key Points:
1) Custom jawline implants can have disproportionate enlargements of the jaw angles compared to the chin based on the patient’s aesthetic desires.
2) In patients with strong masseter muscle attachments and who only need jaw angle width, a custom jawline implant can be designed around the ligamentous attachments to avoid the risk of masseteric muscle dehiscence.
3) Adequate subperiosteal dissection over and behind the masseteric ligamentous attachments are needed for proper placement of a non-ligamentous released jaw angle implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon