

Background: Bridge of the nose deficiencies are a common nasal shape concern and are usually congenital in origin. Occasionally it may also develop from nasal impaction injuries. A most origin of nasal bridge depression is from brow bone augmentation. As the frontonasal junction projection is increased as part of the brow bone augmentation the radix of the nose below it will appear lower. Whether that causes a significant radix deficiency depends on how much brow bone projection the implant creates as well as whether some radix deficiency existed before the brow bone augmentation.
When building up the upper part of the nose, whether a brow bone implant exists above it or not, a variety of augmentation techniques can be used. The most common method would be cartilage grafts, septal cartilage grafts for small radix augmentation and rib cartilage for more major bridge and dorsal line augmentations. Implants may also be used and a variety of standard silicone and ePTFE implants are available to do so.
The rarest form of nasal augmentation of any amount is with a custom implant design. Its use would be indicated if the patient wants a precise preoperatively determined nasal implant shape or that the augmentation requires a precise implant shape to it. Getting a precise fit up against a custom brow bone implant with a border base at the implant junction which narrows as it descends over the nasal bones would fulfill the criteria of the need for a precise implant shape.
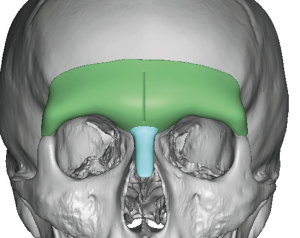
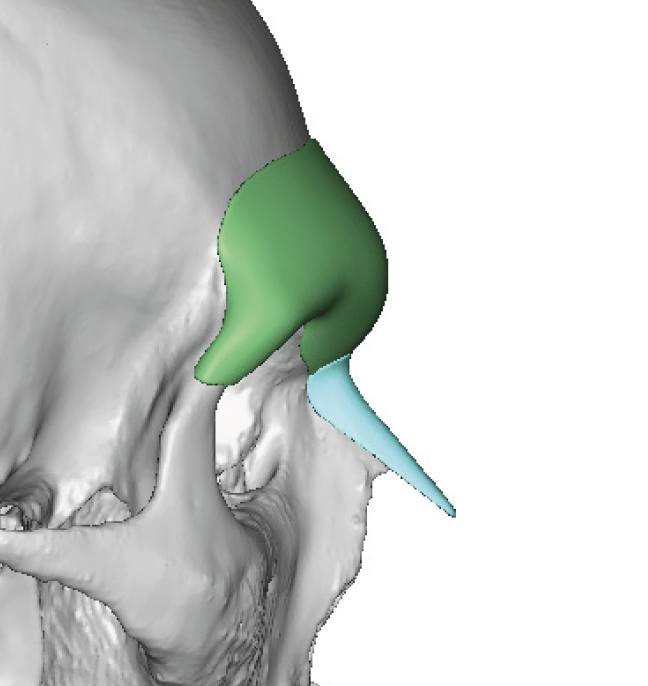
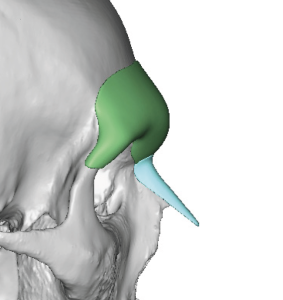 Case Study: This male had a prior custom brow bone implant placed several years previously. He returned wanting to extend the augmentation from the frontonasal area onto the nose and requested a custom implant design to do so. Using his prior brow bone implant design file a custom nasal implant was designed to build up the radix of the nose.
Case Study: This male had a prior custom brow bone implant placed several years previously. He returned wanting to extend the augmentation from the frontonasal area onto the nose and requested a custom implant design to do so. Using his prior brow bone implant design file a custom nasal implant was designed to build up the radix of the nose.

 While its implant volume was small (1cc) its shape was very precise with a broader upper footplate to fit upon against the brow bone implant.
While its implant volume was small (1cc) its shape was very precise with a broader upper footplate to fit upon against the brow bone implant.

 Under general anesthesia for other procedures the implant was placed. Its high position up against the brow bone implant can be seen when placed on the outside.
Under general anesthesia for other procedures the implant was placed. Its high position up against the brow bone implant can be seen when placed on the outside.

 An open rhinoplasty was used for its placement as having a direct linear dissection upon to the brow bone implant high in the pocket was done. It was felt to be better than an intranasal closed technique. He also had a prior open rhinoplasty so a columellar scar was already present. Once the pocket was developed the implant was coated with Vancomycin antibiotic powder.
An open rhinoplasty was used for its placement as having a direct linear dissection upon to the brow bone implant high in the pocket was done. It was felt to be better than an intranasal closed technique. He also had a prior open rhinoplasty so a columellar scar was already present. Once the pocket was developed the implant was coated with Vancomycin antibiotic powder.

 His immediate intraoperative results show adequate augmentation of the upper nose with a more gradual transition at the frontonasal junction.
His immediate intraoperative results show adequate augmentation of the upper nose with a more gradual transition at the frontonasal junction.
The custom nasal implant is the least frequently performed of all custom facial implant designs. The obvi0us reason is that a variety of autologous and implant options exists that do well in the relatively non-complex anatomy of the bridge of the nose. In a straight line of variable thicknesses intraoperative sharing of grafts and implants are almost always adequate. But in the rare instance of a specific nasal ‘defect’ from a prior custom brow bone implant designing a secondary frontonasal augmentation provides the most predictable outcome.
Key Points:
1) Brow bone augmentation can potentially make the radix of the nose look deeper.
2) To build up the upper 1/3 of the bone to blend into a brow bone implant a custom nasal implant design can be used.
3) A custom nasal implant is placed through an open rhinoplasty approach to ensure midline positioning.
Dr. Barry Eppley
World-Renowned Plastic Surgeon