

Background: Midface augmentation is a general term that could affect any of the number of bony surfaces that make up the middle third of the face. The infraorbital rims and maxilla provide anterior augmentation surfaces for forward projection while the zygomatic body and arch provide lateral augmentation surfaces for adding midface width.
By far the most common aesthetic midface augmentation effect has been for zygomatic anterolateral projection because of the use of standard cheek implants. But the use of custom implant designs has made every conceivable type of midface augmentation change possible. Being able to bring the whole midface forward is one of those changes that has only been possible in the past through complex bony osteotomies. But such changes now are possible in a more effective and less invasive manner provided it is not necessary to move the position of the upper teeth forward.
The most common custom midface implant in my experience is the infraorbital-malar design. These designs are used to create the high cheekbone look as well as improve congenital infraorbital deficiencies such as those associated with negative orbital vectors. While effective in doing so some patients may desire even further infraorbital rim augmentation. In so doing it then becomes important to augment the entire midface bone surfaces below to avoid having the rim look like a step off arm the deficient bone below it.
 Case Study: This male had a history of successful custom infraorbital-malar implants done two years previously. He decided he wanted additional augmentation not only of the infraorbital rims but of the entire maxilla beneath it.
Case Study: This male had a history of successful custom infraorbital-malar implants done two years previously. He decided he wanted additional augmentation not only of the infraorbital rims but of the entire maxilla beneath it.
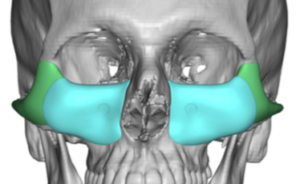
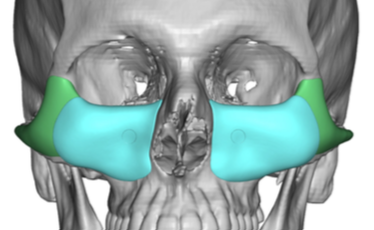
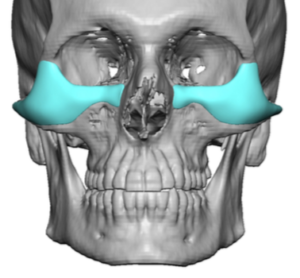
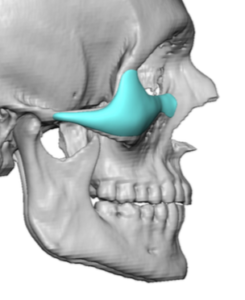
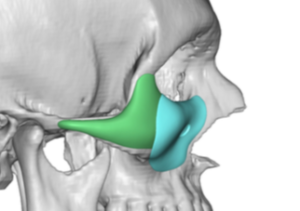 Custom infraorbital-maxillary implants were designed aided by his previous implant designs. There was a significant overlay of the new implants up over and onto the previous implant’s infraorbital rims. A circular mark was made in the implant’s design for the location of the infraorbital nerves.
Custom infraorbital-maxillary implants were designed aided by his previous implant designs. There was a significant overlay of the new implants up over and onto the previous implant’s infraorbital rims. A circular mark was made in the implant’s design for the location of the infraorbital nerves.

 Through re-opening of his previous lower eyelid incisions and new intraoral incisions a complete subzerosteal tissue elevation was done on the midface. The implants were prepared by cutting out the location of the infraorbital nerves and making a slit in the material above it across the infraorbital rim.
Through re-opening of his previous lower eyelid incisions and new intraoral incisions a complete subzerosteal tissue elevation was done on the midface. The implants were prepared by cutting out the location of the infraorbital nerves and making a slit in the material above it across the infraorbital rim.

 The implants were inserted intraorally and pass up around the nerve onto the infraorbital rim. The visible location of the split in the implant overlay confirmed a successful pass around the nerve. Double screw fixation was applied from through the lower eyelid as well as through the mouth.
The implants were inserted intraorally and pass up around the nerve onto the infraorbital rim. The visible location of the split in the implant overlay confirmed a successful pass around the nerve. Double screw fixation was applied from through the lower eyelid as well as through the mouth.
 Closure of the superior approach was done by figure-of-eight cheeklifts and lateral canthopexies. The intraoral incisions was closed in two musculomucosal layers.
Closure of the superior approach was done by figure-of-eight cheeklifts and lateral canthopexies. The intraoral incisions was closed in two musculomucosal layers.
It is not rare that augmentation of one facial area can lead to the desire for a greater augmentation effect later. This is known as ‘accomplishment feedback’. When one procedure is successful it can motivate one to enhance the effect of the first procedure. In this case a more complete midface augmentation effect was achieved by overlaying the original implant. In effect making the two stage implant cover more of the entire deficient midface bone.
Case Highlights:
1) The midface augmentative effect achieved from prior infraorbital-malar implants can be further enhanced by the placement of custom infraornital-maxillary overlay implants.
2) Overlay custom infraorbital-maxillary implants are placed using a combined lower eyelid and intraoral incisions.
3) The key in its placement is navigating around the infraorbital nerve through implant modification.
Dr. Barry Eppley
Indianapolis, Indiana