

Background: The effects of deformational plagiocephaly are most significantly seen on the back of the head. This is not surprising as most of the potential deformation comes from either how the fetus is positioned in utero or how the baby lies after birth. While not conclusively proven, although a biologically sound theory, is that the more significant flattened back of the heads probably have an in utero origin as this is a very malleable and prolonged period of skull formation.
In significant flattenings of the back of the head there are always associated shape deformations around it. Most commonly the contralateral side of the head can have a more protrusive shape. It may look very protruding because of the opposite flatter side or it may even be slightly more prominent than normal. In addition the ipsilateral temporal area is flatter as a wrap around effect from the flattened back of the head. The crown or top of the heads may well be higher than normal as well.
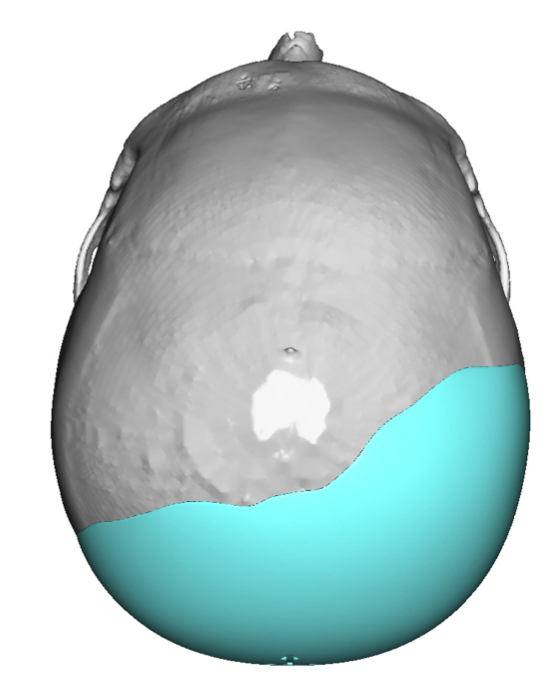
All of these associated deformations must be factored into the skull implant design used to treat it. From the top view the implant should create a symmetrical head shape that is equal on both sides. The implant must extend far enough forward onto the temporal area to match the other side. While in design files the implant may look like it is sitting on bone. But in actuality the implant will ultimately sit on top of the temporal muscle which is not visualized on a 3D bony CT scan. If the top of the head is too high it is important to not have the implant go top to meet it too avoid making the head even higher. It can be decided whether the higher top of the head should be lowered (which will require a separate incision) or to just leave it alone and have the implant stop short of it.
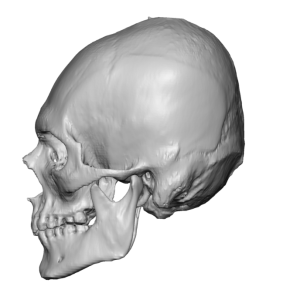
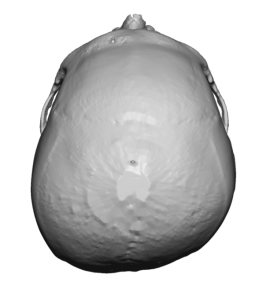 Case Study: This male had a congenital very flat back of his head. Now that he was getting older and his hair thinner he wanted a better back of the head shape. His 3D CT scan showed an asymmetric back of the head with right-sides flattening and a shortened front to back head length.
Case Study: This male had a congenital very flat back of his head. Now that he was getting older and his hair thinner he wanted a better back of the head shape. His 3D CT scan showed an asymmetric back of the head with right-sides flattening and a shortened front to back head length.
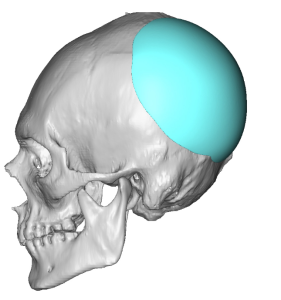
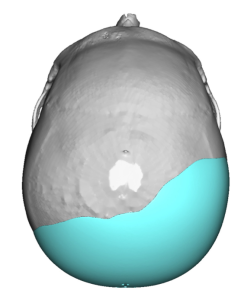 His custom skull implant design had a maximum projection of 15mms on the flatter side with a total volume of 133ccs.
His custom skull implant design had a maximum projection of 15mms on the flatter side with a total volume of 133ccs.

 Under general anesthesia and in the prone position, a wavy horizontal scalp incision was made over the nuchal ridge. Through this incision subperiosteal undermining was done over the entire back of his head, anteriorly on the deep temporal fascia and onto the top of the head. The implant was then rolled rolled for insertion, unrolled and positioned as per the design and secured by two microscrews. A two layer scalp closer was done over a drain.
Under general anesthesia and in the prone position, a wavy horizontal scalp incision was made over the nuchal ridge. Through this incision subperiosteal undermining was done over the entire back of his head, anteriorly on the deep temporal fascia and onto the top of the head. The implant was then rolled rolled for insertion, unrolled and positioned as per the design and secured by two microscrews. A two layer scalp closer was done over a drain.

 His intraoperative changes in the shape of his head were immediately apparent and significant.
His intraoperative changes in the shape of his head were immediately apparent and significant.

 When seen the next day for head dressing and drain removal the change in the shape of his head was even more dramatic in the context of seeing his entire head.
When seen the next day for head dressing and drain removal the change in the shape of his head was even more dramatic in the context of seeing his entire head.
Case Highlights:
1) Significant plagiocephaly involves flattening on one side of the back of the head that extends to involve the ipsilateral temporal area as well.
2) The custom skull implant used to treat such back of the head plagiocephalies are often wider than they are tall… a design feature that must be factored into their placement.
3) The effects of a custom skull implant for a flat back of the head are aesthetically significant, improving the golden ratio of the head in profile.
Dr. Barry Eppley
World-Renowned Plastic Surgeon