

Background: The skull is prone to a wide variety of aesthetically undesired shapes from areas of flatness to excessive prominences. Many of these appear in specific patterns and can be given descriptive names by their presentation. Some are associated with an adjoining suture line. While congenital craniosynostoses skull deformities are the most well known they are also fairly rare and cause more severe skull deformities. Conversely aesthetic skull shape issues are far more common and their deformities are less severe although still disturbing to the patient.
One of these aesthetic skull deformities is known as the coronal dip so named because of its anatomic association with the coronal suture line. There is a transverse linear indentation or dip across the top of the head. This palpable dip is particularly seen in profile and disrupts the normally smooth upper sagittal skull line in profile. This is particularly noticeable in the shaved head male with an obvious shape deformity. Many times the coronal dip occurs in isolation. But as all skull bones and suture lines are connected it is no surprise there may be skull shape concerns.
While the isolated coronal dip is a ‘small’ skull shape issue a custom skull implant is still the best way to treat it. But if other skull areas need simultaneously treated then a much larger skull implant can be designed to treat it.
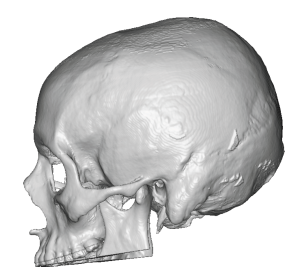
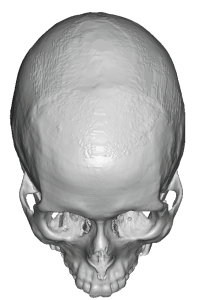 Case Study: This male was bothered by the dip across the top of his head as well as some upper back of the head flatness, which was most manifest on the right. Although he had a full head of hair he did not like the way his head looked when he had a much shorter hairstyle. His 3D skull CT scan showed the coronal dip in profile as well as in the front views.
Case Study: This male was bothered by the dip across the top of his head as well as some upper back of the head flatness, which was most manifest on the right. Although he had a full head of hair he did not like the way his head looked when he had a much shorter hairstyle. His 3D skull CT scan showed the coronal dip in profile as well as in the front views.
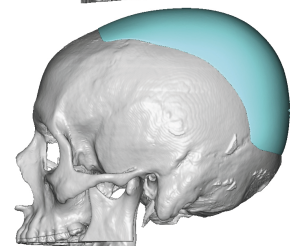
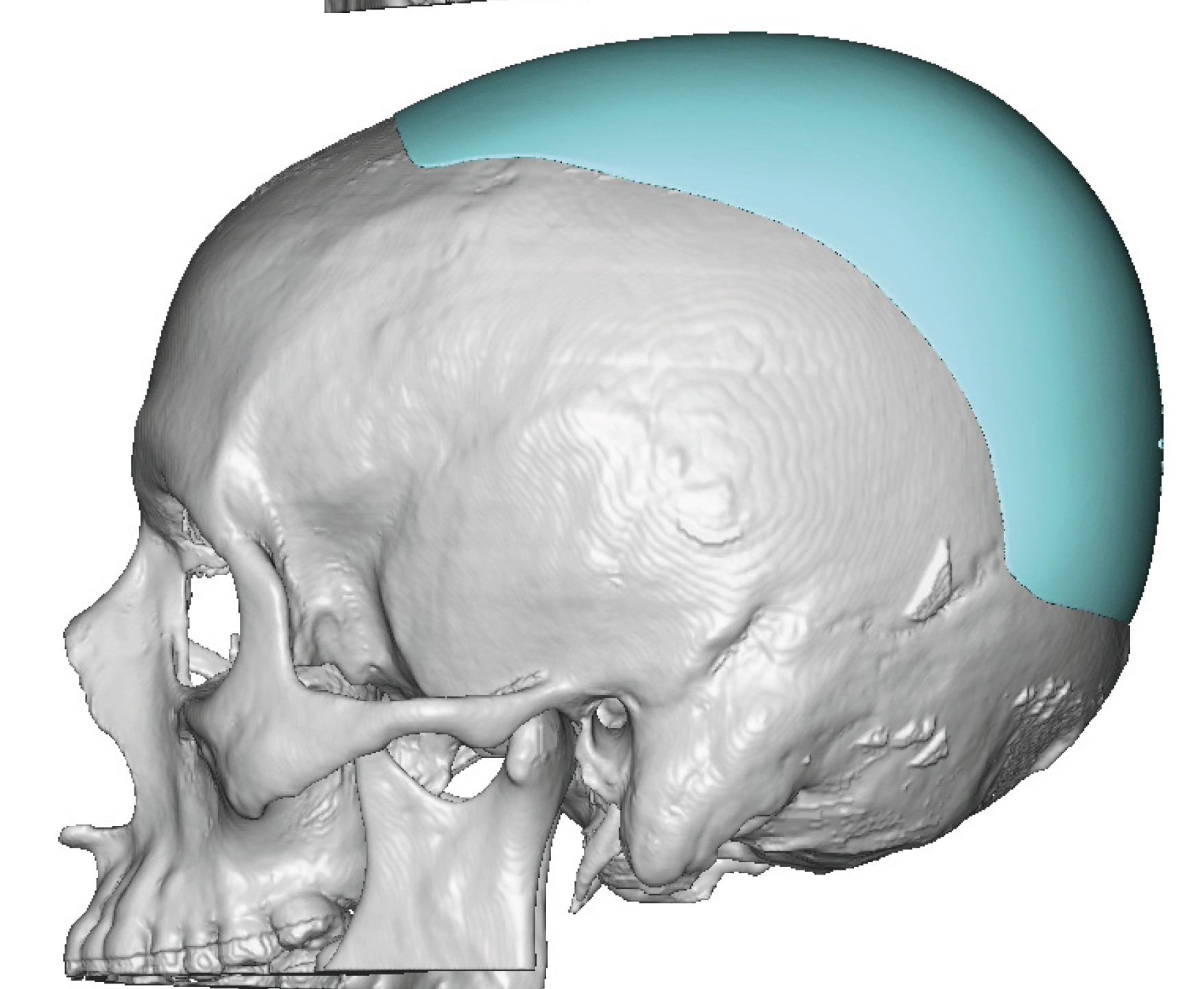
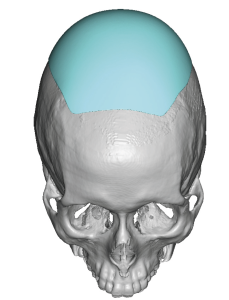 A custom skull implant was designed that not only corrected the coronal dip but also extend to the back to add volume as well as correct the asymmetry. The implant volume was 90ccs.
A custom skull implant was designed that not only corrected the coronal dip but also extend to the back to add volume as well as correct the asymmetry. The implant volume was 90ccs.

 Under general anesthesia and through a scalp incision on the back of the head the custom skull implant was placed in one piece. To aid the dissection and implant placed around the corner (crown of the skull) all the way to the frontal hairline a small additional incision was made more anteriorly. This permitted not only the subperiosteal dissection to be successfully completed but also provided a point of access to make sure the anterior edge of the implant was adequately unfolded.
Under general anesthesia and through a scalp incision on the back of the head the custom skull implant was placed in one piece. To aid the dissection and implant placed around the corner (crown of the skull) all the way to the frontal hairline a small additional incision was made more anteriorly. This permitted not only the subperiosteal dissection to be successfully completed but also provided a point of access to make sure the anterior edge of the implant was adequately unfolded.
 Screw fixation was applied and the incision closed over a drain.
Screw fixation was applied and the incision closed over a drain.

 The improvement in his head shape profile could be appreciated at the end of the surgery.
The improvement in his head shape profile could be appreciated at the end of the surgery.
The cause of a coronal dip is unknown although it must be related to the suture line. Perhaps it is a microform of coronal synostosis although the opposite effect should occur with a raised coronal suture line if that was the case. Regardless it is a distinct indentation across the coronal suture line in a transverse orientation and, having seen it numerous times, it is related to the development of the skull somehow. It is a distinct and small indentation in terms of volume and it is tempting to do something ‘simple’ to treat it such as bone cement or sheets of ePTFE. But it covers a bigger area that one thinks and having all edges blend perfectly into the surrounding bone is no small task. Thus a custom implant design is the best way to effectively augment it. The need for a custom implant design becomes imperative when another area of the skull is concurrently being augmented.
Key Points:
- 1) The coronal dip skull deformity is a linear indentation or dip at or along the coronal suture line across the top of the head. It may also be associated with flattening at the upper back of the head as well.
2) In profile the coronal dip creates a disruption in the smooth sagittal line across the top of the head near its median axis.
3) The coronal dip deformity is best treated by a custom skull implant which could be isolated to it only or could have a broader skull coverage if other areas needed contoured as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon