

Background: The skull is an overall oblong shape that has five distinct surfaces to it. (front, back , top and two sides) The main anatomic ‘dividing line’ between all of these surface of the bony temporal line. This is a distinct raised ridge of bone that starts at the tail of the brow bone anteriorly and extends along the side of the head until it reaches the back of the head. It exists because it is the broad origin of the temporalis muscle. What that means from a surface area standpoint is that it is the dividing line between the top and side of the head. (as well as the front and back of the head as well)
The shape of the skull is prone to a wide variety of asymmetries, almost all of which involve more than one of its five surface areas. This is typified by asymmetries of the top of the head which can involve the sagittal, parasagittal and the temporal line. Almost all parasagittal skull deficiencies cross the bony temporal line or at least have a flatter temporal line than the opposite side. The relevance of that anatomy is that the skull augmentation needed to correct it must partially be on bone but, as it crosses the bony temporal line, must transition onto the top of the muscle. (deep temporal fascia) This again shows that almost all skull asymmetries involve at least two skull surfaces due to its natural convex shape.
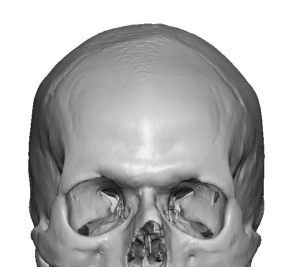
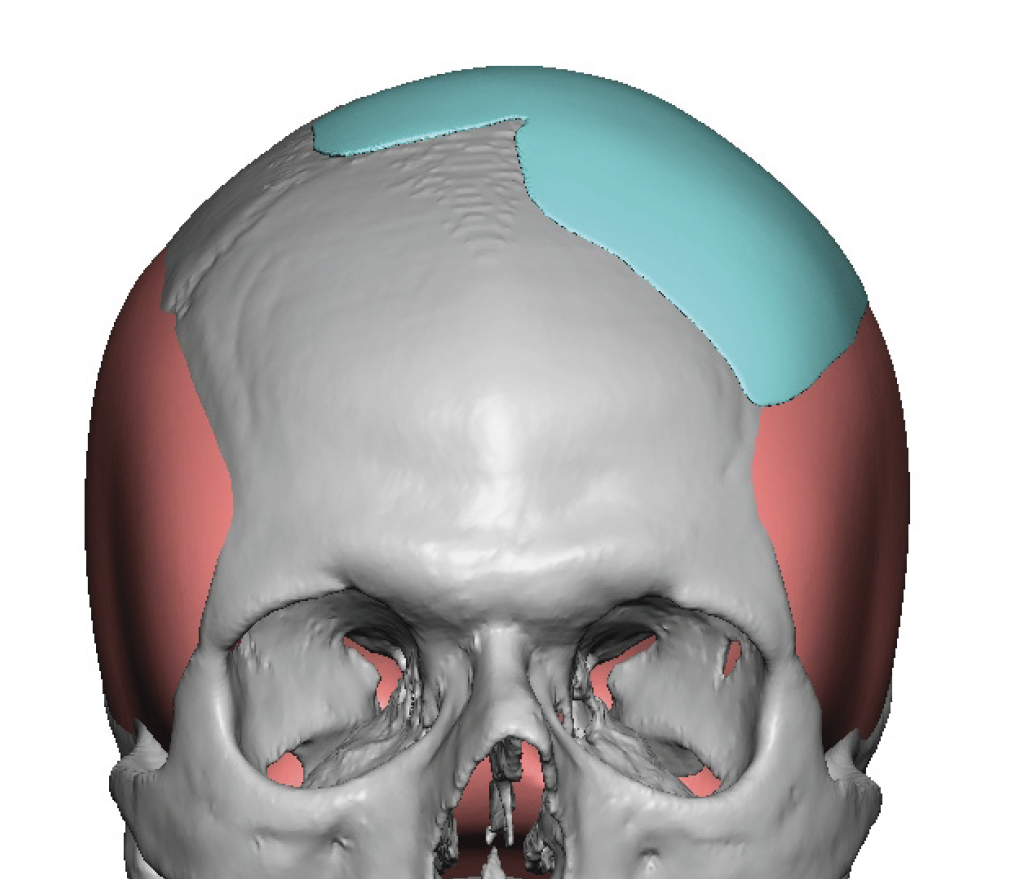
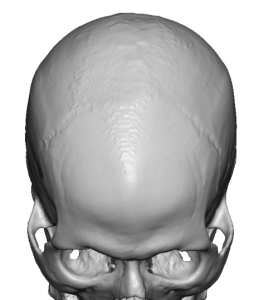 Case Study: This male had been bothered for a long time with the left-sided asymmetry of the top of his head. On his ‘bucket list’ was the goal to one day undergo its correction. His 3D CT scan clearly showed this asymmetry with the lower and laterally displaced bony temporal line.
Case Study: This male had been bothered for a long time with the left-sided asymmetry of the top of his head. On his ‘bucket list’ was the goal to one day undergo its correction. His 3D CT scan clearly showed this asymmetry with the lower and laterally displaced bony temporal line.
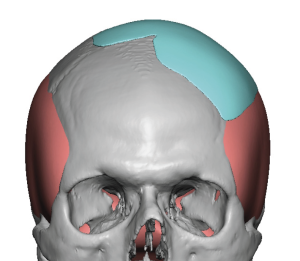
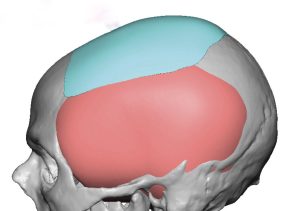 Using his 3D CT scan a custom left parasaggital-upper temporal implant was designed too mirror that of the shape of the other side.There was a very small section of the design that crossed over the midline to augment a small sagittal ridge depression that he saw.
Using his 3D CT scan a custom left parasaggital-upper temporal implant was designed too mirror that of the shape of the other side.There was a very small section of the design that crossed over the midline to augment a small sagittal ridge depression that he saw.



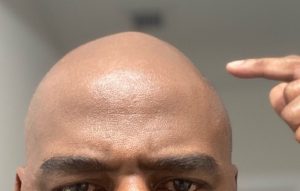
 Prior to the surgery an outline of the implant was marked on the scalp along with the incision location. (In red) Under general anesthesia a 3cm scalp incision was made and the implant pocket developed. The implant was then inserted, positioned and secured with two small titanium micro screws. A multilayer scalp closure was done after placement of a drain.
Prior to the surgery an outline of the implant was marked on the scalp along with the incision location. (In red) Under general anesthesia a 3cm scalp incision was made and the implant pocket developed. The implant was then inserted, positioned and secured with two small titanium micro screws. A multilayer scalp closure was done after placement of a drain.
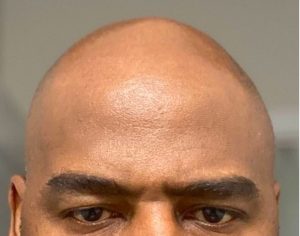
 When seen the next day for head dressing and drain removal the improvement in top of the head symmetry was seen.
When seen the next day for head dressing and drain removal the improvement in top of the head symmetry was seen.
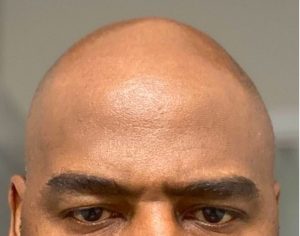
Some skull asymmetries can be more modest or subtle while others are more significant in size. Many of the more modest skull asymmetries present in the shaved head male patient where the smooth and completely exposed scalp can be seen. Between the full exposure and the light reflections off of the scalp even minor skull asymmetries can be aesthetically bothersome. While any size for surface area skull implant can be designed it is of equal importance that it is capable off being placed through the smallest possible scalp incision. The smaller the skull augmentation the more important it is that the scalp incision to treat it is equally small. This case illustrates that exact point with the placement of a skull implant through an incision that does not even seem possible.
Case Highlights:
1) One unique type of skull asymmetry involves the top of the head along the parasagittal and upper temporal regions.
2) The top of the head is separated from the side of the head by the bony temporal line of which a parasagittal skull deficiency often crosses that line when the top of the head is asymmetric.
3) A custom skull implant of a discrete thickness can be designed and placed for top of head asymmetries.
Dr. Barry Eppley
Indianapolis, Indiana