

Background: Asymmetry of the back of the head, often called plagiocephaly, is a deformational skull deformity. The flatness on one side of the back of the head is its hallmark sign and is a common reason patients present for aesthetic skull implants. The source is largely congenital in nature (in utero) although there can be some significant contribution from a deformational contribution after birth.
Traumatic and medically-induced plagiocephalies, meaning influenced by an internal cause, would be very rare. Skull fractures, repaired or not, would be an example of traumatic plagiocephaly where the fractured bone if it occurs at an early age affected its growth. Medically induced plagiocephaly refers to a surgical procedure done during development (e.g., craniotomy) where the invasive surgery and applied fixation has affected the growth of the bone in the region of the contour deformity.
Healed craniotomy bone flaps are certainly rare to see in the aesthetic skull reshaping patient, particularly in the region of the deformed skull. But what is even more rare is a VP shunt associated with it. Its management as well as the fixation hardware in the implant’s design for augmentation of the deformed bone is of interest.
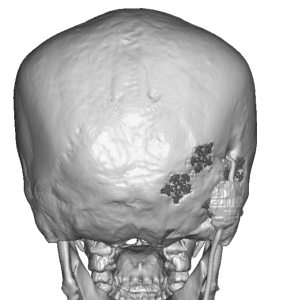
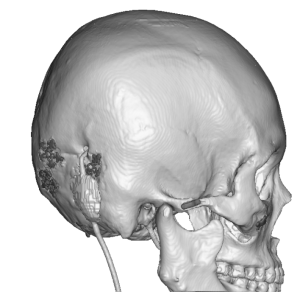 Case Study: This female desired to have the overall flatter back of her head improved in projection with correction of the flatter right side. She had a significant prior medical history of a right occipital craniotomy for a benign brain tumor done when she was younger in which a VP shunt was placed for temporary CSF drainage. Despite being done over a decade ago the VP shunt remained in place although it was believed to be non-functional. Her 3D CT scan showed a significant brachycephaly with mild occipital flattening on the craniotomy/VP shunt. Given her ethnicity (Asian) she had a natural tendency for brachycephaly which was very evident in the scan.
Case Study: This female desired to have the overall flatter back of her head improved in projection with correction of the flatter right side. She had a significant prior medical history of a right occipital craniotomy for a benign brain tumor done when she was younger in which a VP shunt was placed for temporary CSF drainage. Despite being done over a decade ago the VP shunt remained in place although it was believed to be non-functional. Her 3D CT scan showed a significant brachycephaly with mild occipital flattening on the craniotomy/VP shunt. Given her ethnicity (Asian) she had a natural tendency for brachycephaly which was very evident in the scan.
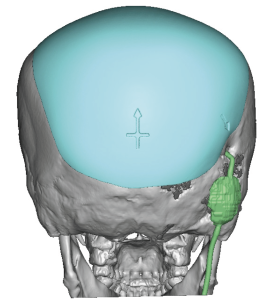
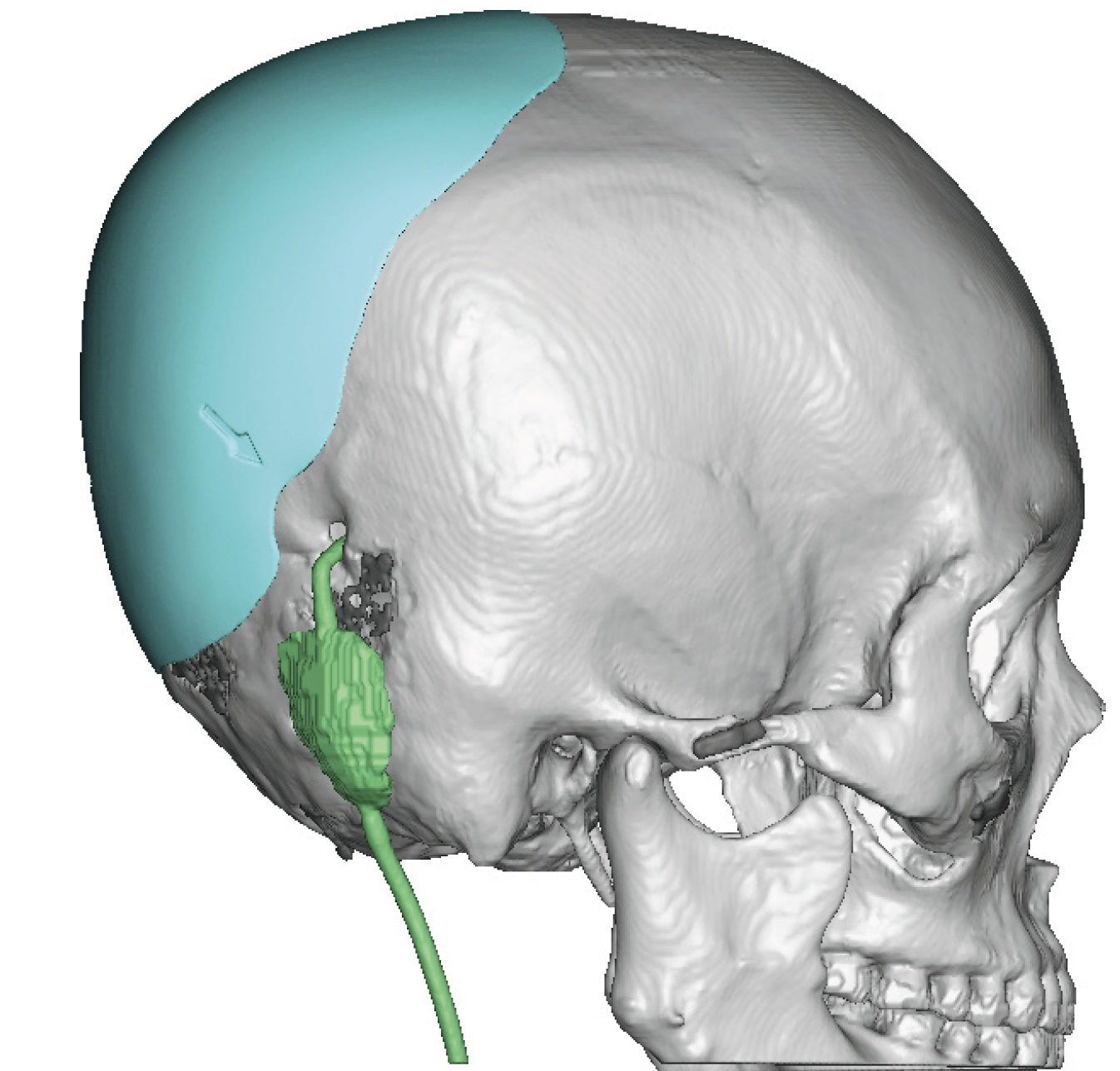
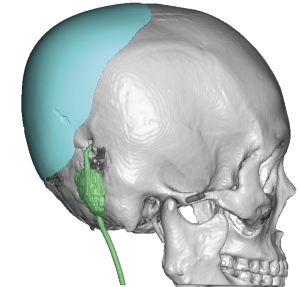 A custom implant was designed for augmentation of the back of the head passing over some of the craniotomy fixation plates but stearing clear of the VP shunt. (even though the flattening involved that area as well)
A custom implant was designed for augmentation of the back of the head passing over some of the craniotomy fixation plates but stearing clear of the VP shunt. (even though the flattening involved that area as well)
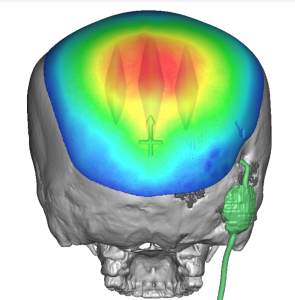 As seen in the colored thicknesses of the implant design the goal was to create some brachycephaly improvement while also correcting the more flat right side…as much as possible but avoiding the VP shunt. The central thickness of the implant was 16mms with a volume of 126ccs.
As seen in the colored thicknesses of the implant design the goal was to create some brachycephaly improvement while also correcting the more flat right side…as much as possible but avoiding the VP shunt. The central thickness of the implant was 16mms with a volume of 126ccs.

 Under general anesthesia and in the prone position her existing right scalp scar from her craniotomy was used for access. It was opened, the lateral fixation plate exposed and the entire scalp elevated off of the back of the head.
Under general anesthesia and in the prone position her existing right scalp scar from her craniotomy was used for access. It was opened, the lateral fixation plate exposed and the entire scalp elevated off of the back of the head.

 The custom skull implant was prepared by placing multiple 4mm perfusion holes, inserted into the pocket and positioned by using how it laid over the fixation plate. The arrow on the implant design showed its reference to the VP shunt location.
The custom skull implant was prepared by placing multiple 4mm perfusion holes, inserted into the pocket and positioned by using how it laid over the fixation plate. The arrow on the implant design showed its reference to the VP shunt location.
 Over a drain the scalp was closed in multiple layers with resorbable sutures.
Over a drain the scalp was closed in multiple layers with resorbable sutures.

 The intraoperative side by side of the before and after showed the increase in back off head projection.
The intraoperative side by side of the before and after showed the increase in back off head projection.
Brachycephaly is commonly seen for augmentation of the flat back of the head of which many such patients are Asian in ethnicity. Asymmetry is not that common in brachycephaly and it is clear that the prior craniotomy has some effect in that regard. While it is perfectly safe to cover the fixation plates the VP shunt should obviously be avoided even though it was presumed to be non-functional.
The prior craniotomy has its advantages and disadvantages. The scalp provides a convenient location of access without creating a new scalp scar. How the craniotomy will cause some restriction to scalp expansion and this needs to figured into the implant design.
Key Points:
1) A prior craniotomy can be a source of skull asymmetry particularly if it was performed during development.
2) An indwelling VP shunt in the area off skull asymmetry does not prevent the placement of a custom skull implant.
3) An existing scalp scar can serve as access for the placement of a custom skull implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon