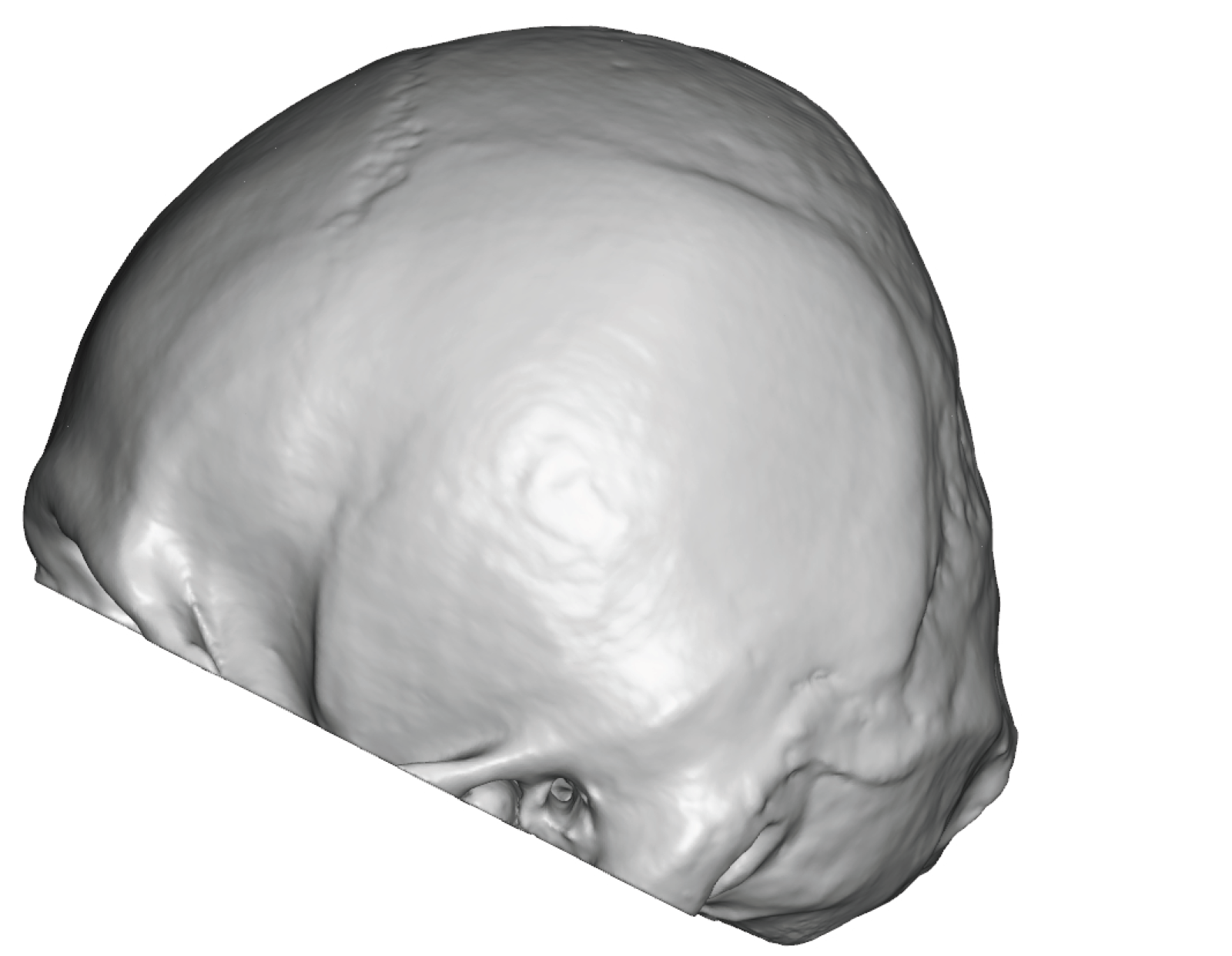


 Background: The flat back of head is a result of inadequate projection of the occipital-parietal bones. The lower half of the visible back of the head is the location of the upper half of the occipital bone. (the lower half of the occipital bone is below the thick neck muscles) The upper half of the back of the head is the location of the paired parietal bones which unite in the middle along the sagittal suture line. The occipital and parietal bones are separated by the lambdoid suture line. Of no anatomic relevance but interesting is that the sagittal and lambdoid sutures create a Mercedes sign on the back of the head.
Background: The flat back of head is a result of inadequate projection of the occipital-parietal bones. The lower half of the visible back of the head is the location of the upper half of the occipital bone. (the lower half of the occipital bone is below the thick neck muscles) The upper half of the back of the head is the location of the paired parietal bones which unite in the middle along the sagittal suture line. The occipital and parietal bones are separated by the lambdoid suture line. Of no anatomic relevance but interesting is that the sagittal and lambdoid sutures create a Mercedes sign on the back of the head.
As a result of these complex bone and suture components of the back of the head and the forces to which it is exposed, but in utero and postnatal, it is no surprise that flattening deformations of its shape occurs. Such contour depressions take on many forms which fall into three general categories; 1) unilateral flatness/asymmetry, 2) bilateral flatness and 3)upper/parietal/crown flattening. While all of these back of head contour flatteninmgs can be improved, the more complete (bilateral) head flattening poses the biggest challenge in getting an optimal increased contour projection.
With bilateral flattening the projection of back of the head is barely beyond the posterior bony temporal lines in profile. Such flattening is associated within tight scalp since it is always congenital in origin. How much projection can be achieved with a custom skull implant is not controlled by the implant design but by how much the scalp can stretch to accommodate it.
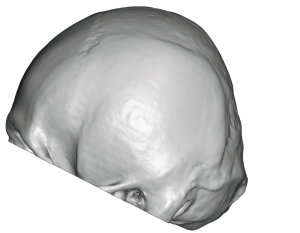
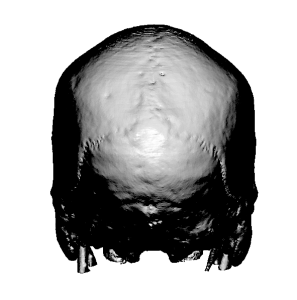
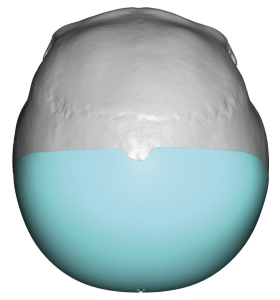
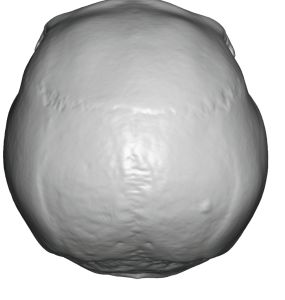 Case Study: This male had a completely flat back of his head which would be judges as severe as evidenced both by external appearance as well as his 3D CT scan. On the scan the flattened contour barely extended beyond the bony projection of the posterior temporal lines in side view. In top view the flattened contour sat inside the bony temporal lines.
Case Study: This male had a completely flat back of his head which would be judges as severe as evidenced both by external appearance as well as his 3D CT scan. On the scan the flattened contour barely extended beyond the bony projection of the posterior temporal lines in side view. In top view the flattened contour sat inside the bony temporal lines.
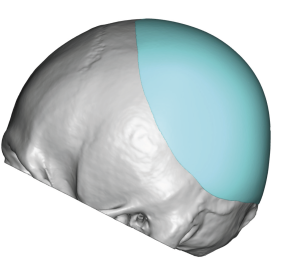
 A custom back of head skull implant was designed that added 15mm of central projection and 155ccs of implant volume. This was felt to be the maximum size of implant that could safely fit without undue pressure on the elevated scalp.
A custom back of head skull implant was designed that added 15mm of central projection and 155ccs of implant volume. This was felt to be the maximum size of implant that could safely fit without undue pressure on the elevated scalp.

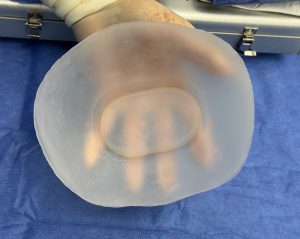 Under general anesthesia and in the prone position the custom skull implant was placed through a low horizontal scalp incision. Its design incorporated an internal ring of material relief to help with its placement.
Under general anesthesia and in the prone position the custom skull implant was placed through a low horizontal scalp incision. Its design incorporated an internal ring of material relief to help with its placement.

 The intraoperative change was evident with a visible improvement in the back of the head projection.
The intraoperative change was evident with a visible improvement in the back of the head projection.

 When seen the next day for drain removal the improved back of head projection was just as visible.
When seen the next day for drain removal the improved back of head projection was just as visible.
While this skull implant provided a good amount of projection with high volume you may have been expecting an even bigger change. Snd although we all would have liked more it is the maximal change that could be safely done with the amount of scalp stretch available. Hopefully for him he will find it satisfactory and can leave his flat head concerns behind. If. not he can always have a secondary skull augmentation where the implant volume can be increased another 50%. He also could have had a first stage scalp expansion to get a much larger implant but most men do not find the scalp expansion process very appealing.
Key Points:
1) The flat back of the head presents in varying contour flattening but in the most severely affected the projection of the occipital bone is not much greater than the posterior bony temporal line.
2) The degree of bone flattening affects how much increased back of head projection is possible with scalp stretch limitations.
3) Optimal back of head augmentations often require a two stage approach but most males are not usually enthusiastic about the use of a scalp tissue expander.
Dr. Barry Eppley
World-Renowned Plastic Surgeon