

Background: The skull is prone to a wide variety of shape malformations by virtue of its multiple suture connections during development. Premature fusion of these sutures cause well known forms of head deformity known as craniosynostoses. While these classic forms of craniosynostosis are the result of near or complete premature fusion of these suture lines there are greater numbers of people who are affected by lesser degrees of suture line fusion. As a result they present with less severe head shape deformities but ones that are aesthetically distressing nonetheless.
One such lesser craniosynostosis variant head shape deformity is that of the peaked or triangular head shape. Rather than a rounder top of the head from front and back views it is shaped more like an inverted V. Its appearance suggests a high sagittal ridge, which in some more minor cases may be true, but more often is due to parasagittal skull deficiencies. Lateral to the sagittal suture the skull has not fully expanded. This can also appreciated by the more inward positioning of the temporal line…contributing to an overall narrow head shape.
Rounding up and out the peaked head shape is the key to getting an improved head shape. There may be a slight need to reduce the sagittal ridge but this is not going to make a major change in head shape. It is the augmentation of the deficient sides that makes the more important aesthetic contribution.
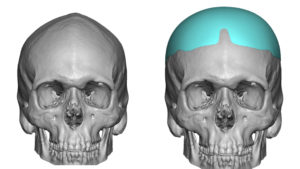
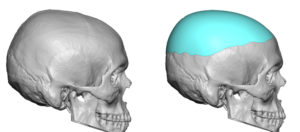
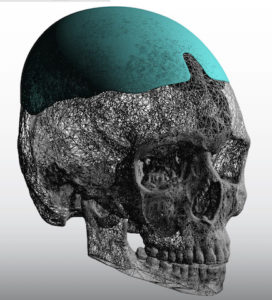
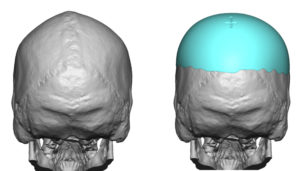 Case Study: This young male who shaved his head had a peaked head shape marked by a pseudo sagittal ridge, significant bilateral parasagittal and temporal line defiiency and an upper back of the head flattening. From his 3D CT scan a custom skull implant was deigned to reshape the entire top of his head. Feathering the implant into the forehead is the hardest part of the design to ensure that the augmentation covers what is needed but does not go lower than needed into the thinner tissues of the forehead.
Case Study: This young male who shaved his head had a peaked head shape marked by a pseudo sagittal ridge, significant bilateral parasagittal and temporal line defiiency and an upper back of the head flattening. From his 3D CT scan a custom skull implant was deigned to reshape the entire top of his head. Feathering the implant into the forehead is the hardest part of the design to ensure that the augmentation covers what is needed but does not go lower than needed into the thinner tissues of the forehead.
 Under general anesthesia and through a limited scalp incision, the implant needed to be placed. Despite the elastic deformation properties of the implant even that would not permit it to be passed through the idea short scalp incision length.
Under general anesthesia and through a limited scalp incision, the implant needed to be placed. Despite the elastic deformation properties of the implant even that would not permit it to be passed through the idea short scalp incision length.
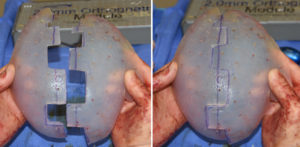
 It was then decided to split the implant is half using a geometric split technique. This would ensure that when put back together inside the scalp pocket that there would be an assured re-assembly that was both precise and structurally stable. Each half of the implant was passed through the incision and then ‘snapped’ back together. It was held together by sutures and screw fixation to the bone in the part of the implant that can seen through the incision..
It was then decided to split the implant is half using a geometric split technique. This would ensure that when put back together inside the scalp pocket that there would be an assured re-assembly that was both precise and structurally stable. Each half of the implant was passed through the incision and then ‘snapped’ back together. It was held together by sutures and screw fixation to the bone in the part of the implant that can seen through the incision..
 His immediate intraoperative results shows a significant head shape improvement. This was more of a shaping skull implant, with the parasagittal thickness being no greater than 8mms, than it was an enlarging skull implant.
His immediate intraoperative results shows a significant head shape improvement. This was more of a shaping skull implant, with the parasagittal thickness being no greater than 8mms, than it was an enlarging skull implant.
Beyond the need for an improved head shape, it is also important to not create an undue scar burden as well. This requires some innovative thought into how it can be placed with the scar length in mind.
Case Highlights:
1) A peaked head shape deformity is when the height of the skull has a prominent sagittal ridge with parasagittal deficiency.
2) Creating a rounder head shape requires requires primary augmentation of the parasagittal skull deficiency which is best done with a custom skull implant.
3) To limit the length of the scalp scar in men with shaved head a geometric split implant insertion technique is needed.
Dr. Barry Eppley
Indianapolis, Indiana