

Background: Flat areas on the skull are one of the primary indications for the use of custom skull implants. While flat skull areas can occur anywhere on the skull they have a propensity to be more on the back of the head than anywhere else. This is undoubtably due to that the back of the head gets pressed on more than any other skull area during in utero development as well as after birth. (particularly after birth) As a result part or all of the back of the head may not have a symmetrical convex shape to it.
Flatness of the back of the head affects men and women equally. More men seek correction of it because of greater exposure of it due to less hair coverage. But while most women have and retain more hair to camouflage flat skull areas this does not mean they are not aware of it. Females are motivated to seek correction when either they tire of working with their hair to cover it, their hair becomes thinner or they just desire to have an enhanced head shape.
 One way to think about flatness on the back of the back of the head is its north-south or vertical involvement. Using the lambdoidal suture line as a north-south indicator does the flatness involve the occipital bone below the suture line, the parietal bones above the suture line or both. While men are often bothered by back of head flatness that significantly affects the occipital bone, women are often more bothered by flatness at a higher level over the parietal bones closer to the crown of the skull.
One way to think about flatness on the back of the back of the head is its north-south or vertical involvement. Using the lambdoidal suture line as a north-south indicator does the flatness involve the occipital bone below the suture line, the parietal bones above the suture line or both. While men are often bothered by back of head flatness that significantly affects the occipital bone, women are often more bothered by flatness at a higher level over the parietal bones closer to the crown of the skull.
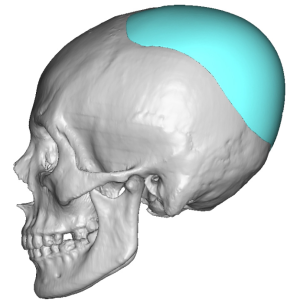
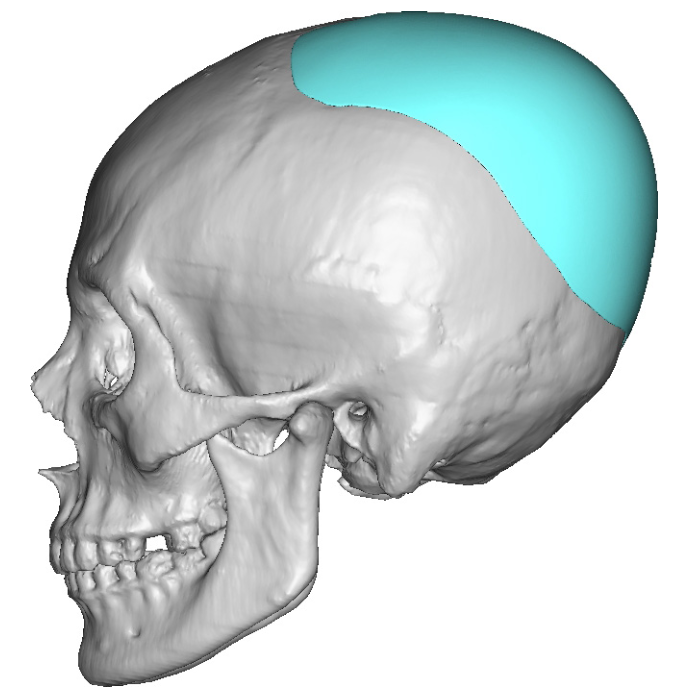
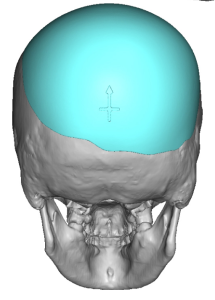 Case Study: This female was bothered by the flat back of her head higher up near the crown area. She also had sone mild asymmetry of the flatness of the back of her head with the right being a bit flatter than the left. Using her 3D CT skull scan a custom implant design was made to augment the flat skull areas. A maximum central projection of 15mm was made creating a total implant volume of 141ccs.
Case Study: This female was bothered by the flat back of her head higher up near the crown area. She also had sone mild asymmetry of the flatness of the back of her head with the right being a bit flatter than the left. Using her 3D CT skull scan a custom implant design was made to augment the flat skull areas. A maximum central projection of 15mm was made creating a total implant volume of 141ccs.

 Under general anesthesia and in the prone position a low horizontal scalp incision was used to access the entire back and top of the head to create a subperiosteal pocket. The implant was prepared by placing multiple 4mm perfusion holes with a dermal punch.
Under general anesthesia and in the prone position a low horizontal scalp incision was used to access the entire back and top of the head to create a subperiosteal pocket. The implant was prepared by placing multiple 4mm perfusion holes with a dermal punch.
 The implant was inserted and positioned in the midline. It was so tight that it was very difficult to even move it around inside the pocket. Which proves that the maximum implant volume had been chosen.
The implant was inserted and positioned in the midline. It was so tight that it was very difficult to even move it around inside the pocket. Which proves that the maximum implant volume had been chosen.
 After the placement of a drain over the implant the scalp was closed in multiple layers with dissolvable sutures.
After the placement of a drain over the implant the scalp was closed in multiple layers with dissolvable sutures.

 Her immediate intraop results showed the improvement in the shape of the back of her head.
Her immediate intraop results showed the improvement in the shape of the back of her head.
In designing skull implants, back of the head included, the most important design question is volume. How much volume of the implant is needed to create the desired augmentation effect? That is important for more than the desired effect as certain implant volumes can not be placed due to the limited stretch of the scalp. For those patients not desiring a two stage skull augmentation approach it is important to try and push the implant volume in the design as much as possible. For most patients this is close to 150ccs.
Case Highlights:
1) Flat back of the head skull deformities occur in females as well as men but often are more crown focused.
2) The scalp can tolerate implant volumes up to 150ccs with immediate insertions dependent on the thickness of the scalp.
3) A low occipital scalp incision is used to insert and position the skull implant per its design.
Dr. Barry Eppley
World-Renowned Plastic Surgeon