

Background: In pediatric craniofacial surgery one of the most known procedures is that of cranial vault reconstruction. Done for craniosynostosis and other severe congenital skull deformities, it involves the extensive removal of misshapen skull bones and their immediate reconstruction in infants and very young children. The success of these procedures is based on the remarkable bone forming ability of the underlying dura which only exists at very young ages.
While many infantile cranial vault reconstructions heal well, a full and complete skull thickness and shape does not always occur. Irregularities and partial bony defects are not rare. And in some cases small full-thickness bony defects may also persist. Numerous factors exists as to why the skull doesn’t heal completely including the extent of the bone removal, what size bone defects were left after reconstruction and the age of the patient when the surgery was done.
Some adults with skull contour defects after cranial vault surgery done in the first year or so after birth do present for secondary contour restoration. Their reconstruction options include and complete reopening of their scalp flap and application of bone cement or the placement of a custom skull implant done through a potentially smaller scalp incisional approach.
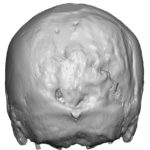
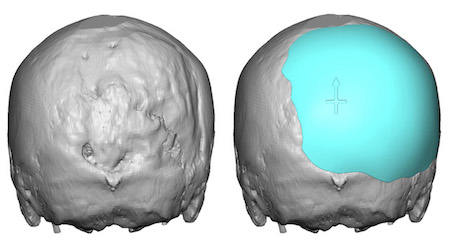
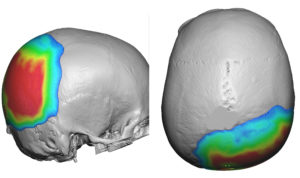
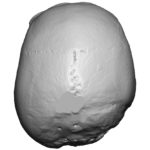 Case Study: This young man presented for contouring of a right occipital skull defect. He had long been bothered by it since his teenage years. He started he had some form of skull surgery as an infant but was unclear as to why it was done. He had a large horseshoe-shaped scalp on the occiput. Using a 3D CT scan the extent of his right occipital skull defect could be appreciated with a very irregular skull contour and a few areas of full-thickness defects.
Case Study: This young man presented for contouring of a right occipital skull defect. He had long been bothered by it since his teenage years. He started he had some form of skull surgery as an infant but was unclear as to why it was done. He had a large horseshoe-shaped scalp on the occiput. Using a 3D CT scan the extent of his right occipital skull defect could be appreciated with a very irregular skull contour and a few areas of full-thickness defects.
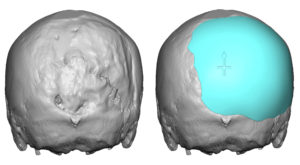
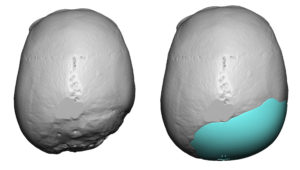 Using his 3D CT scan a custom occipital skull implant was designed to match the contour of the other side. The design implant had a maximum thickness of 8mms with a total volume of 85ccs
Using his 3D CT scan a custom occipital skull implant was designed to match the contour of the other side. The design implant had a maximum thickness of 8mms with a total volume of 85ccs
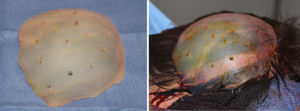
 Under general anesthesia and in the prone position, the right side of his old scalp incision was opened only. Careful scalp tissue elevation was necessary to avoid potential dural violation. In the areas of known full-thickness defects dissection was done slightly above the bone surface leaving extra soft tissue over these areas. The skull implant had multiple perfusion holes placed and it was then inserted, positioned and screwed into place.
Under general anesthesia and in the prone position, the right side of his old scalp incision was opened only. Careful scalp tissue elevation was necessary to avoid potential dural violation. In the areas of known full-thickness defects dissection was done slightly above the bone surface leaving extra soft tissue over these areas. The skull implant had multiple perfusion holes placed and it was then inserted, positioned and screwed into place.

 The immediate effects of the skull implant were apparent with the creation of a symmetric back of the geared with a smooth contour. He ultimately viewed the result the day after surgery as ‘life-changing’.
The immediate effects of the skull implant were apparent with the creation of a symmetric back of the geared with a smooth contour. He ultimately viewed the result the day after surgery as ‘life-changing’.
 In the properly selected prior cranial vault surgery patient who has no or limited full-thickness skull defects, a custom skull implant can be both an effective and safe secondary reconstructive technique.
In the properly selected prior cranial vault surgery patient who has no or limited full-thickness skull defects, a custom skull implant can be both an effective and safe secondary reconstructive technique.
Case Highlights:
1) Infant cranial vault surgery can result in long-term skull contour issues due to partial and full thickness bony defects.
2) A 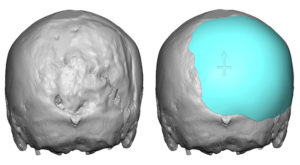 is the best approach if a limited scalp incision is to be used for contour restoration.
is the best approach if a limited scalp incision is to be used for contour restoration.
3) Careful elevation of scalp tissues for implant placement from previous areas of skull surgery must be done in areas of known full-thickness bone defects.
Dr. Barry Eppley
Indianapolis, Indiana