

Background
A narrow head shape in adults can only be corrected through implant augmentation. The most critical design consideration is whether the implant should remain within the bony temporal line or extend beyond it.
-
Type 1 Implants augment only the sides of the head and stay within the temporal lines.
-
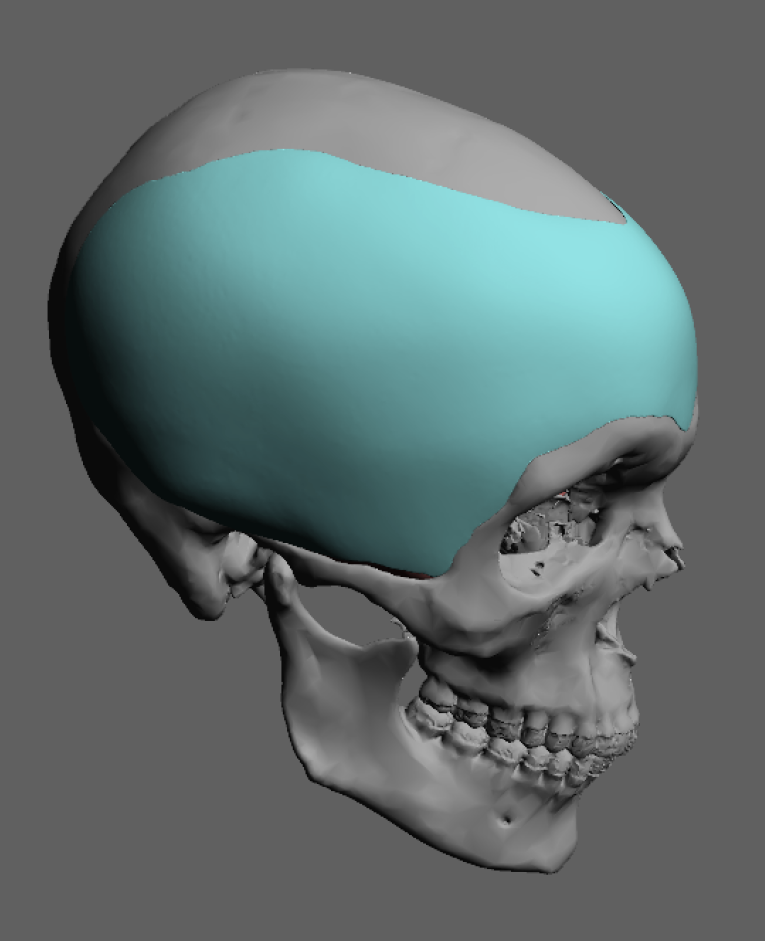
Type 2 Implants—used for more severe narrowness—wrap around the head, crossing the temporal lines to reach the forehead and/or back of the skull.
The narrower the head, the more likely a Type 2 wrap-around design will be necessary.
Anatomic Considerations
The bony temporal line serves as the attachment point for the temporalis muscle and its deep fascial covering. While it technically comprises a superior (fascial) and inferior (muscular) ridge, the distinction is often subtle.
-
For Type 1 implants, augmentation can be placed beneath the deep temporal fascia or even under the muscle. The submuscular location is generally preferred.
-
In Type 2 cases, the implant must cross the temporal line, making submuscular placement unfeasible. The fascia and muscle insertions should never be detached, as they cannot be adequately re-draped over an implant and tend to retract.
Thus, for wrap-around skull implants, the design must accommodate:
-
Subperiosteal placement on the forehead and occiput
-
Subfascial (on top of the deep fascia) placement on the sides
This ensures a smooth and continuous contour.
Case Summary
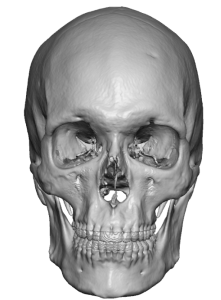
 This male patient presented with a clinically narrow head shape, more pronounced in person than on 3D CT scans.
This male patient presented with a clinically narrow head shape, more pronounced in person than on 3D CT scans.
Design and Planning
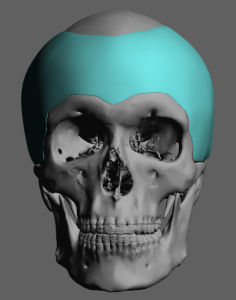
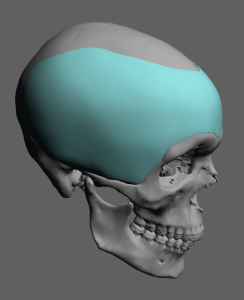 A custom wrap-around skull implant was created to augment the forehead and both sides of the head. Due to its size and surface area, the implant was designed as a two-piece segment, split along the midline of the forehead.
A custom wrap-around skull implant was created to augment the forehead and both sides of the head. Due to its size and surface area, the implant was designed as a two-piece segment, split along the midline of the forehead.
Surgical Technique
A three-incision approach was used:
-
Bilateral postauricular incisions to pass the implants
-
Frontal hairline incision for central access and alignment
Each incision served a distinct role: the postauricular incisions allowed access for lateral insertion, while the frontal incision was essential for joining the two pieces at the forehead.
Implant Insertion

 Although it may seem difficult to insert such a large implant through small incisions, the material’s deformability allowed it to be folded, inserted, and then re-expanded within the pocket.
Although it may seem difficult to insert such a large implant through small incisions, the material’s deformability allowed it to be folded, inserted, and then re-expanded within the pocket.
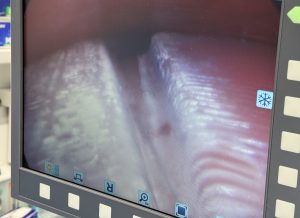 Joining the two segments in the forehead was technically demanding due to limited visibility. A combination of endoscopic visualization and external palpation was used to align them. Despite best efforts, a 2mm separation remained between the segments.
Joining the two segments in the forehead was technically demanding due to limited visibility. A combination of endoscopic visualization and external palpation was used to align them. Despite best efforts, a 2mm separation remained between the segments.
 To prevent a visible gap, a 1mm sheet of ePTFE was placed over the junction.
To prevent a visible gap, a 1mm sheet of ePTFE was placed over the junction.
Postoperative Course
-
All incisions were closed with resorbable sutures.
-
Drains were placed bilaterally and left in for over two weeks.
-
Needle aspiration was performed several times for minor fluid collections after drain removal.
-
By three weeks, fluid accumulation had resolved.
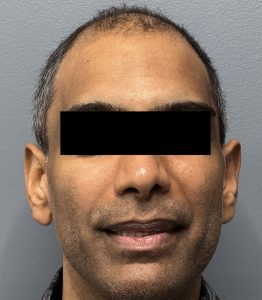
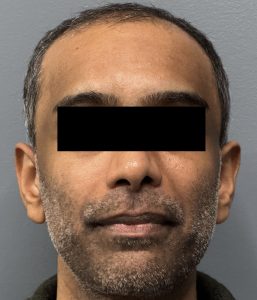 The result showed significant head width improvement and a more balanced cranial shape. Final evaluation of any implant edging will require additional time.
The result showed significant head width improvement and a more balanced cranial shape. Final evaluation of any implant edging will require additional time.
Clinical Insights
Augmenting skull areas that involve the temporal zones requires extra care to preserve muscular soft tissues. This makes wrap-around implant placement more complex than standard onlay augmentations.
Risks and Management
-
Implant edging and fluid buildup are common concerns, especially when implants lie over the temporal muscle.
-
These risks are mitigated through:
-
Careful implant design
-
Prolonged drain placement
-
However, the most unique challenge remains the intraoperative insertion of a large, segmented implant through limited-access incisions under semi-blinded conditions.
Key Takeaways
-
Effective correction of narrow head shapes requires crossing the temporal line, combining subperiosteal and subfascial placement techniques.
-
Strategic incisions behind the ears and along the frontal hairline allow for hidden access and precise assembly.
-
Large surface area implants demand segmentation and internal reassembly, which must be done with precision and finesse.
Dr. Barry Eppley
World-Renowned Plastic Surgeon