

Background: The clavicle is the well observed bone that sits horizontally between the shoulder and the sternum. But despite its seemingly simple assignment the anatomy of its shape is far more complex than most would think given what it exists to do. It has the most obvious function of attaching the upper arm to the trunk via the shoulder girdle. As a result it transmits forces from the upper arm to the axial skeleton which is what helps creates its complex shape. Lastly, and often under appreciated, is that it provides protection of the major blood vessels and nerves that supply the upper arm.
These three clavicular bone assignments create a surprisingly complex shape that is initially appreciated given its lazy s-shaped or sigmoid shape. But within this shape of the bone is how its thickness changes which is a function of the loads that it bears. The inner 1/3 of the clavicle is the thickest part in the 20mm range from one outer cortex to the other. Conversely it is thinnest near the shoulder joint at the outer third at the 12 to 14mm range. The middle third has thickness that lies between the two in the 14 to 16mm range. These bone thicknesses are particularly relevant when it comes to plate fixation of fractures and osteotomies so complete bicortical screw engagement is achieved at each fixation site.
But what is also interesting about these varying bone thicknesses along the length of the clavicle, which is not as relevant in fracture repair, is that in reduction osteotomies two dissimilar thicknesses of the clavicle are what is put back together. One would think that a segment of 2.5cm in length would not create such dissimilar size but it does. The outer clavicle diameter ends up being about 2/3s that of the inner clavicle diameter. While these two clavicle ends heal 99.5% of the time (I have had 1 non-union in 200 clavicle reduction osteotomies) it does pose the question of whether of the hardware is removed does this represent a weak spot along the length of the clavicle…or does it continue to remodel over time and eventually eliminate the step-off between the two ends?
Case Study: This female desired a shoulder feminization procedure with a bideltoid distance of 48cms and a square shoulder appearance.

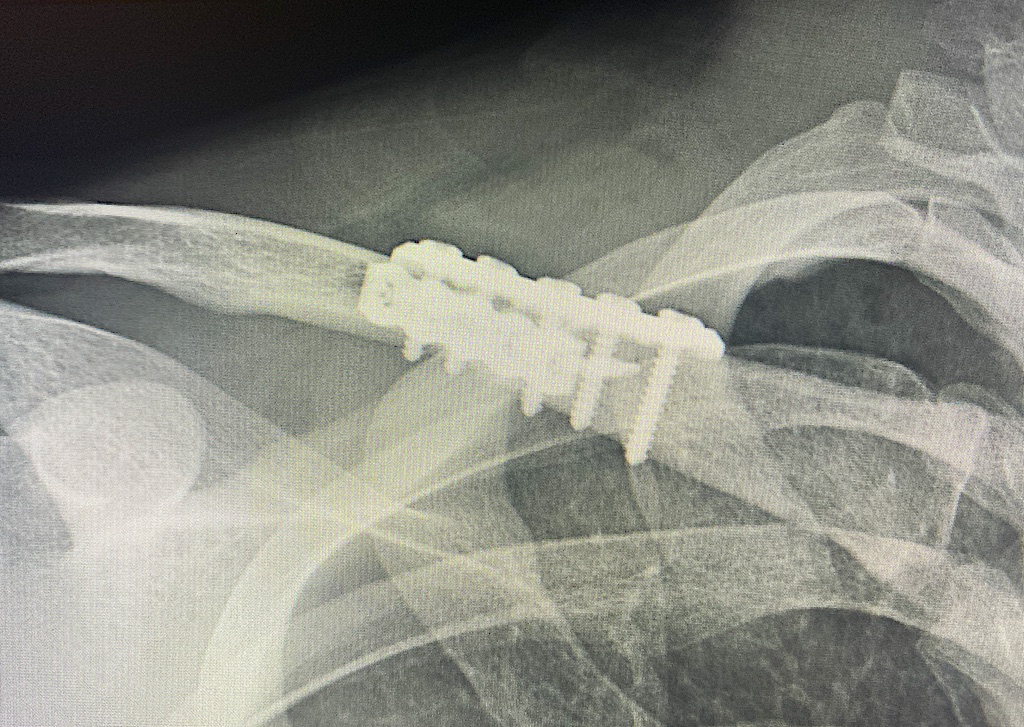
 Under general anesthesia bilateral clavicle reduction osteotomies were performed at the inner third of the clavicles. A 2.5cm segment of bone was removed from each side with double plate fixation with bicortical screw placements.
Under general anesthesia bilateral clavicle reduction osteotomies were performed at the inner third of the clavicles. A 2.5cm segment of bone was removed from each side with double plate fixation with bicortical screw placements.
 Postop x-rays show confirmation of bicortical screw placement with 20mms screw lengths medially and 16mm screw lengths laterally.
Postop x-rays show confirmation of bicortical screw placement with 20mms screw lengths medially and 16mm screw lengths laterally.

 The 2 day after surgery results show the change in shoulder width in the front view. The incisions are closed with small dissolvable sutures and covered with flesh-colored tapes that will remain in placed for weeks after the surgery
The 2 day after surgery results show the change in shoulder width in the front view. The incisions are closed with small dissolvable sutures and covered with flesh-colored tapes that will remain in placed for weeks after the surgery
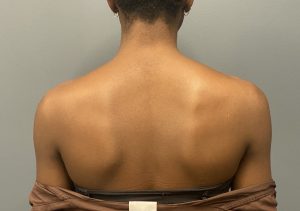
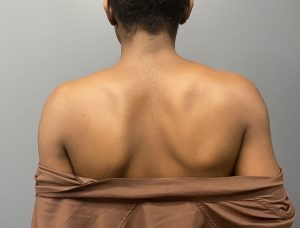 The back view is always the most interesting and not commonly seen since most before and afters focus on the more important front view. I don’t this back view is representative of what a well healed result looks like as the gown is not dropped down low enough and is providing some restriction of a relaxed shoulder posture.
The back view is always the most interesting and not commonly seen since most before and afters focus on the more important front view. I don’t this back view is representative of what a well healed result looks like as the gown is not dropped down low enough and is providing some restriction of a relaxed shoulder posture.
As for the dissimilar clavicle ends when the resected clavicle is brought back together it is only potentially relevant if the hardware is ever removed. The healed osteotomy site may represent a ‘weak’ point because of the change in natural bone thickness. Whether this would be an actual issue is not known given that so few patients to date have ever elected to have their hardware removed.
Key Points:
1) Shoulder narrowing surgery removes a segment of the clavicle that when put back together has two ends of dissimilar cross-sectional diameters.
2) As a result of two different sized bone segments put back together the bicortical screw lengths on each side of the osteotomy line will be different.
3) The long term effects of a clavicle with uneven ends across a healing osteotomy line are unknown but may be irrelevant if the hardware is never removed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon