


Background: The chin is seen as a relatively ‘simple’ anatomic structure with few risks of any neurovascular or dental complications from surgical implant or osteotomy manipulations. And while this is true from any major medical complications this is not accurate when it comes to aesthetic complications. The relationship of the enveloping soft tissue over the chin bone is an under appreciated relationship and one that is once disrupted it create a number of specific aesthetic issues.
One of the common aesthetic problems in the chin, almost always stemming from prior surgery, is chin pad ptosis. This is a general term that describes a basic disruption of the tight enveloping wrap of the soft tissues around the chin bone. It is important to appreciate that the chin is a solitary projecting point, some with more projection than others. The chin pad is attached to the bone by the mentalis muscle origin (in the concave part of the bone below the tooth roots) as well as the periosteum over its surface and the ligamentous attachments along its lower border.
While the intraoral approach offers a scarless approach to chin surgery it separates most of these soft tissue attachments in exposing the bone. This is not an issue as long as the chin bone/support is increased either by an implant or an advancing osteotomy (either horizontally, vertically or both) as the released soft tissues are expanded. But when the reverse occurs via some form of chin reduction (bone burring, reverse sliding genioplasty, narrowing/verteically shortening osteotomy) a soft tissue redundancy is going to occur. The soft tissue chin pad can contract down circumferentially but the redundant soft tissues do not disappear. This results in a soft tissue-bone mismatch and chin pad sagging occurs.
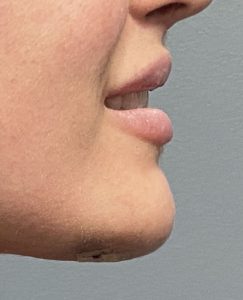
 Case Study: This female underwent a prior intraoral chin reduction procedure by burring with a resultant soft tissue redundancy. At rest this was very subtle but when smiling it became more pronounced. (hyperdynamic chin pad ptosis)
Case Study: This female underwent a prior intraoral chin reduction procedure by burring with a resultant soft tissue redundancy. At rest this was very subtle but when smiling it became more pronounced. (hyperdynamic chin pad ptosis)

 A submental approach was taken for its correction which included a full-thickness soft tissue wedge excision, inferior border muscle tuck and submental defatting. This eliminated the chin pad overhang both at rest and when smiling.
A submental approach was taken for its correction which included a full-thickness soft tissue wedge excision, inferior border muscle tuck and submental defatting. This eliminated the chin pad overhang both at rest and when smiling.



 Her immediate results showed the shape improvement despite the swelling both at rest and in dynamic motion.
Her immediate results showed the shape improvement despite the swelling both at rest and in dynamic motion.
The treatment of chin pad ptosis involves either a superior resuspension or an inferior resection approach. The intraoral resuspension technique has its obvious appeal but is often conceptually flawed as the problem is soft tissue excess not just sagging tissues. This is why a resuspension approach works best when it is combined with some form of added chin support. (implant or osteotomy) As long as there is no associated lower lip sag the submental approach provides assured improvement particularly in dynamic forms of chin ptosis.
Key Points:
1) The soft tissue chin pad can become disinserted from its underlying skeletal support from prior procedures resulting in various amounts of chin pad ptosis.
2) Hyperdynamic chin ptosis is usually associated with a more subtle non-dynamic chin ptosis/excess.
3) Submental excision and chin pad tightening is the definitive treatment for hyperdynamic chin pad ptosis.
Dr. Barry Eppley
World-Renowned Plastic Surgeon