

Background: Chin augmentation using an implant is the most common form of facial augmentation. It has been around for over a half century and is generally thought of a straightforward procedure with a high success rate. And this is true when it is applied for modest chin deficiencies that are associated with no significant lower jaw deficiencies.
As the chin deficiency becomes greater, however, other issues arise that are not seen in more modest chin recessions. Larger chin deficiencies are associated with an overall lower jaw underdevelopment…which means the ramus of the lower jaw is vertically shorter. This makes the horizontal chin shorter but it also makes it vertically longer as the L-shape of the lower jaw is tilted up and back. Thus when placing a large chin implant on the end of the chin bone the augmentation effect is no longer purely horizontal. Some of the horizontal augmentation effect is lost by becoming more vertical, often creating a 30 or 45 degree type of forward chin augmentation effect.
Another interesting effect occurs in short lower jaws that have large chin implants placed…the chin can look out of proportion to the rest of the lower jaw shape. The chin, in essence, becomes ‘over augmented’ while the larger two-thirds of the lower jaw behind it remains structurally deficient. This is what I call ‘chin-jaw’ disproportion’. The surgery has become over focused on the most easily and well known treatable part of it, the chin. The jawline/angles behind it remain narrow and high, often with a high mandibular plane angle with a now protruding chin.
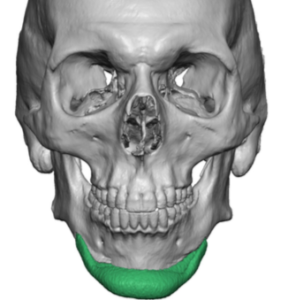
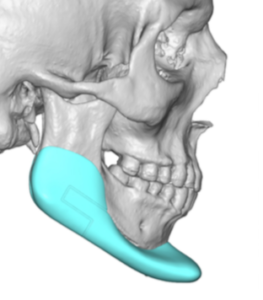
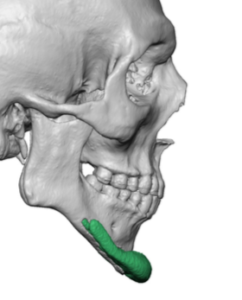 Case Study: This male had a prior history of two successive chin implants placed through a submental incision. Each chin implant created an improved chin augmentation result but he eventually realized that an adequate chin augmentation made the ears of the lower jaw look deficiency with very high and narrow jaw angles. A 3D CT scan showed good placement of the chin implants despite being double stacked and without any rigid screw fixation. His original implanting surgeon did as good a job as was possible with the traditional chin augmentation approach. When augmenting a severely short lower chin the backward slope of the anterior chin bone makes the implants sitting on it sit more at a 45 degree angle, losing some of the forward projection of the implant. This effect becomes magnified the greater the size of the implant augmentation. (in this case using two stacked implants)
Case Study: This male had a prior history of two successive chin implants placed through a submental incision. Each chin implant created an improved chin augmentation result but he eventually realized that an adequate chin augmentation made the ears of the lower jaw look deficiency with very high and narrow jaw angles. A 3D CT scan showed good placement of the chin implants despite being double stacked and without any rigid screw fixation. His original implanting surgeon did as good a job as was possible with the traditional chin augmentation approach. When augmenting a severely short lower chin the backward slope of the anterior chin bone makes the implants sitting on it sit more at a 45 degree angle, losing some of the forward projection of the implant. This effect becomes magnified the greater the size of the implant augmentation. (in this case using two stacked implants)
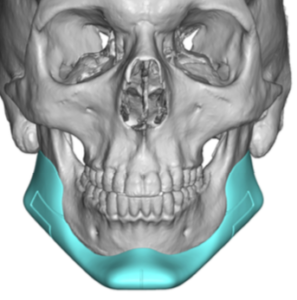
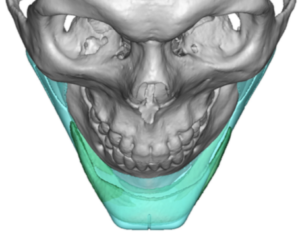
 To create an improved lower facial result that had a more proportionate jaw shape a custom jawline implant design was done incorporating some of the positive features of the two chin implants. (19mm horizontal chin projection) It also eliminated the negative features of excessive vertical lengthening by tilting the chin implant part of the design upward. The jawline part of the design as done to create a connection to the back with some vertical jaw angle lengthening but attention said to not making the jaw angles too wide.
To create an improved lower facial result that had a more proportionate jaw shape a custom jawline implant design was done incorporating some of the positive features of the two chin implants. (19mm horizontal chin projection) It also eliminated the negative features of excessive vertical lengthening by tilting the chin implant part of the design upward. The jawline part of the design as done to create a connection to the back with some vertical jaw angle lengthening but attention said to not making the jaw angles too wide.
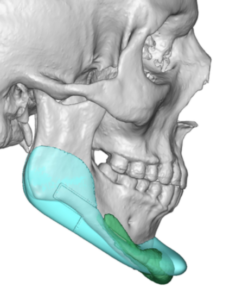
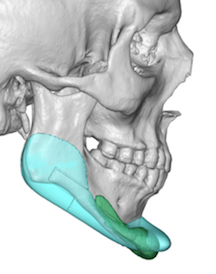
 In digitally overlaying the jawline implant design vs the indwelling chin implants their differences could be seen.
In digitally overlaying the jawline implant design vs the indwelling chin implants their differences could be seen.
 Through the existing submental incision the double stacked chin implants were removed. Capsulectomies were performed on the bone and the bony overgrowths removed by osteotomies. The jaw angle pockets were created through small intraoral posterior vestibular incisions which was connected to the anterior chin dissection. The custom jawline implant was inserted as a single piece in a front to back direction and secured with screws at the chin and jaw angles.
Through the existing submental incision the double stacked chin implants were removed. Capsulectomies were performed on the bone and the bony overgrowths removed by osteotomies. The jaw angle pockets were created through small intraoral posterior vestibular incisions which was connected to the anterior chin dissection. The custom jawline implant was inserted as a single piece in a front to back direction and secured with screws at the chin and jaw angles.
Case Highlights:
1) Large chin augmentations often reveal an underling jaw deficiency by looking disproportionate.
2) Anytime a double-stacked chin implant is used to a sliding genioplasty that exceeds 12 to 14mms this is a sure sign of a significant lower jaw deficiency.
3) A custom jawline implant provides better lower facial proportions between the front and back end of the lower jaw.
Dr. Barry Eppley
Indianapolis, Indiana