

Background: Cheek implants have been around almost as long as chin implants for aesthetic facial augmentations. While over shadowed today in number of procedures performed by filler and fat injections they still have a valuable role to play in aesthetic facial enhancements due to their permanent effects. Their success is based on a variety of factors which includes proper implant style/size selection as well as good surgical placement.
Perhaps unknown to some the genesis of cheek implants was for use in females. You only have to go back to the 30s, 40s and 50s and look at actresses and models to see what was defined as a good female cheek. This was the so called ‘apple cheek’ which is anatomically defined as the malar eminence, the area between the cheekbone and nose in a horizontal orientation and between the eye and the mouth in a vertical orientation. This creates a full or rounded protrusion that has historically been associated with youth and healthiness. It is on his basis cheek implants have been designed. While there are seven different styles of cheek implants they all achieve variations of this apple cheek effect.
While cheek implants have a permanent effect the soft tissues over them can and will change over time. In effect the soft tissues may slide down over the implant. While a cheek implant will have some preventative effects of cheek soft tissue sagging that effect depends the size of the implant and the thickness of the overlying soft tissues.This age-related soft tissue sag an be overcome with a larger implant in both size of its footprint and millimeters of projection.
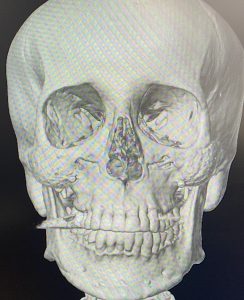
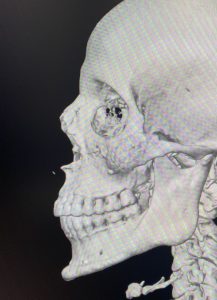 Case Study: This female had a prior history of cheek implants placed intraorally when she was younger. While their effects may have been satisfactory at that time as she has gotten older her cheeks have been more saggy and less full. A 3D CT scan showed the implant location which appeared to be smaller malar style cheek implants secured with a single screw on each side.
Case Study: This female had a prior history of cheek implants placed intraorally when she was younger. While their effects may have been satisfactory at that time as she has gotten older her cheeks have been more saggy and less full. A 3D CT scan showed the implant location which appeared to be smaller malar style cheek implants secured with a single screw on each side.
 Under general anesthesia and through her prior intraoral vestibular mucosal scars the indwelling cheek implants were removed and compared to their replacements. (large malar-submalar style)
Under general anesthesia and through her prior intraoral vestibular mucosal scars the indwelling cheek implants were removed and compared to their replacements. (large malar-submalar style)

 The existing implant pockets were expanded, the new cheek implants placed and secured with single screw fixation.
The existing implant pockets were expanded, the new cheek implants placed and secured with single screw fixation.
 The immediate intraoperative results showed the increased cheek augmentation effect.
The immediate intraoperative results showed the increased cheek augmentation effect.
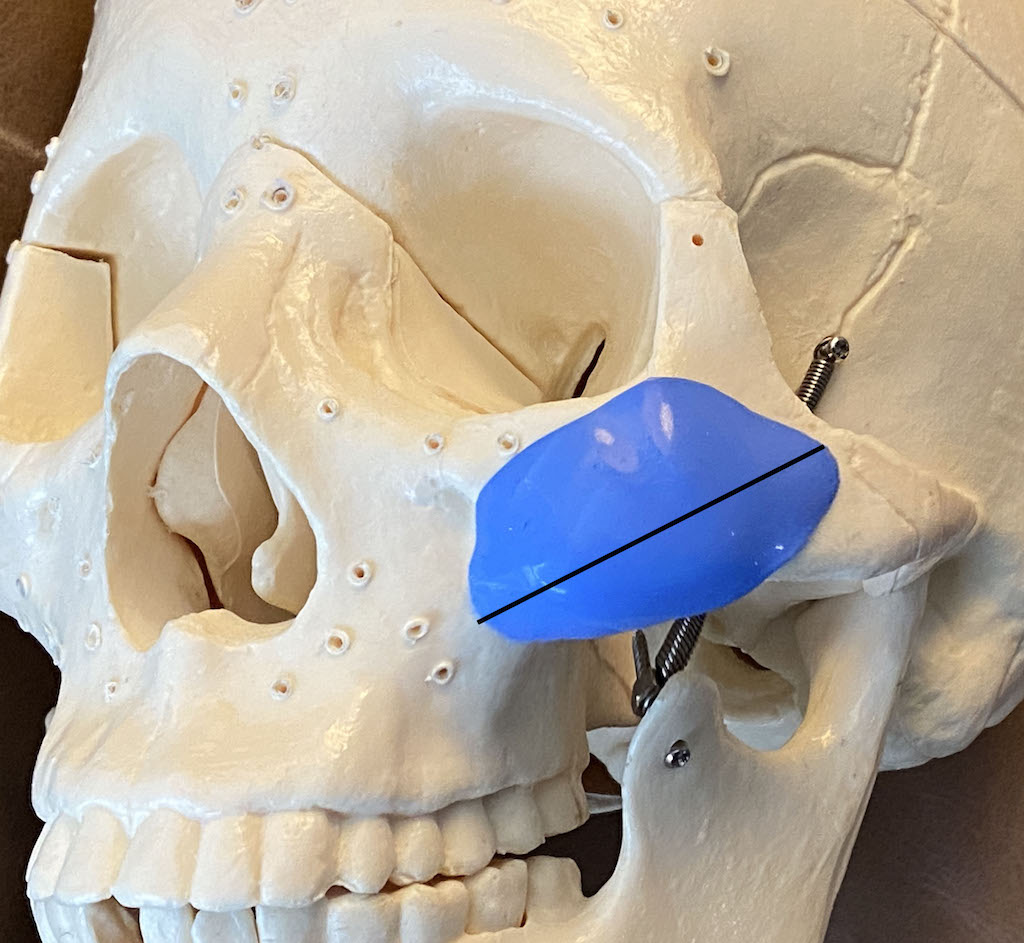
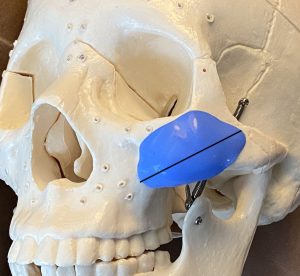 The traditional or standard cheek implant is designed to achieve the apple cheek fullness effect. To do so the implant is designed to have an oblique line of augmentation across what is a more horizontally oriented cheekbone. The main zygomatic body has a convex shape so the implant can cup it with its curved shape. As the implant size gets larger more of the implant will sit onto the masseteric fascia right under the cheekbone. By doing so the soft tissue attachments of the cheek are released…in effect creating a deep plane lift over the cheek area.
The traditional or standard cheek implant is designed to achieve the apple cheek fullness effect. To do so the implant is designed to have an oblique line of augmentation across what is a more horizontally oriented cheekbone. The main zygomatic body has a convex shape so the implant can cup it with its curved shape. As the implant size gets larger more of the implant will sit onto the masseteric fascia right under the cheekbone. By doing so the soft tissue attachments of the cheek are released…in effect creating a deep plane lift over the cheek area.
Case Highlights:
1) Standard cheek implants with ongoing aging may no longer be adequate…or may never have been completely satisfactory even after they were initially placed.
2) To see a more substantial cheek augmentation effect the implant size and footprint have to be substantially increased…often doubling in size.
3) Intraoral placement of standard cheek implants requires partial placement on the masseteric fascia below the bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon