

Background: Chin reduction understandably is the antithesis to chin augmentation. But suffice it to say that a chin reduction is technically harder than a chin augmentation when considering the bone and soft tissue elements involved and isn fraught with its own unique set of challenges. The first one of these is the soft tissue chin pad. When an augmentation is done with an implant or a bony genioplasty there is rarely any soft tissue problems as the chin pad is expanded. In chin reductions, however, what happens to the soft tissue chin pad is an important element in the technique used as reducing its support is no guarantee that it will completely shrink down around a lesser projection of bone. This is why many chin reduction techniques that do not manage the soft tissue as well often develops some degree of chin pad sagging. (ptosis)
The other consideration is how to reduce the excess chin bone projection. High speed burring is the most common technique which can be done through relatively small incisions of which the submental approach is preferred. (as any excess soft tissue can be removed concurrently) When one thinks of osteotomies of the chin the classic sliding genioplasty comes to mind. And while an osteotomy can be done to slide the chin in reverse for reductions this is rarely a good idea as the chin becomes longer as its horizontal projection is decreased, the back ends of the osteotomy will protrude below the inferior border and submental fullness will develop as the soft tissue chin pad excess is redistributed.
Osteotomies can be used in chin reduction as a substitute for burring if a more controlled method of bone removal is desired. It is most useful when the amount of horizontal reduction needed is considerable.
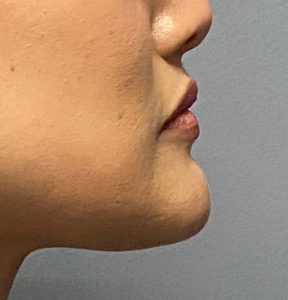 Case Study: This female had a strong jawline and a protruding chin that extended well past a horizontal line dropped down from the lower lip. (7mms) It was also too wide for her aesthetic preference.
Case Study: This female had a strong jawline and a protruding chin that extended well past a horizontal line dropped down from the lower lip. (7mms) It was also too wide for her aesthetic preference.

 Under general anesthesia and through a submental approach the entire projection chin bone was exposed. Using a reciprocating saw a midline cut of 7mms depth was made into the bone.
Under general anesthesia and through a submental approach the entire projection chin bone was exposed. Using a reciprocating saw a midline cut of 7mms depth was made into the bone.

 The saw was then turn 90 degrees from this cut and extended out to the sides. The two pieces were lifted off the bone and removed. The exposed bleeding marrow space was covered with bone wax to stop the bleeding as well as prevent any chance of even minimal regrowth.
The saw was then turn 90 degrees from this cut and extended out to the sides. The two pieces were lifted off the bone and removed. The exposed bleeding marrow space was covered with bone wax to stop the bleeding as well as prevent any chance of even minimal regrowth.

 The chin was lastly narrowed by making angled cuts at the corner to deround the chin and make it more a V bone shape. Excess submental chin pad soft tissues were excised and closed.
The chin was lastly narrowed by making angled cuts at the corner to deround the chin and make it more a V bone shape. Excess submental chin pad soft tissues were excised and closed.

 Her intraoperative results showed the immediate decrease in chin projection.
Her intraoperative results showed the immediate decrease in chin projection.
Larger chin reduction by submental bone removal cane effectively done using a reciprocating saw. Working with a small blade inside a limited submental incision is safer than using a high speed drilll and also allows one to get much further to the sides iof the chin way back beyond the incision. While a saw may mean to some a reversal sliding genioplasty for chin reduction it is an ostectomy technique rather than a traditional osteotomy method.
Case Highlights:
1) Large chin reductions can be done by a submental approach using an osteotomy technique with a small reciprocating saw.
2) For the saw cuts a midline split technique is used which establishes the amount of horizontal projection reduction precisely.
3) With female horizontal chin reductions there usually needs to be side reductions as well to keep the chin from becoming too wide.
Dr. Barry Eppley
World-Renowned Plastic Surgeon