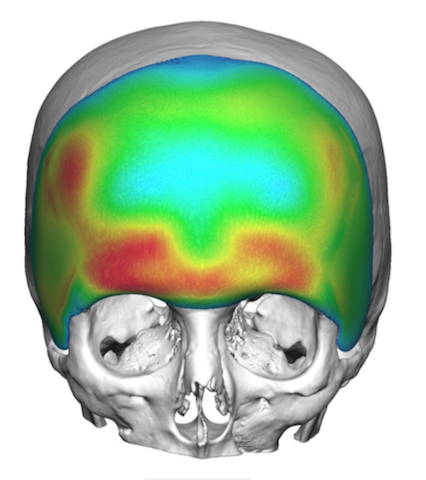


Background: The narrow forehead is often associated with an overall narrow skull shape development. Critical assessment of the narrow forehead shows that it is most restrictive at the temporal lines which indicates it is a combined bony and soft tissue deficiency. Thus augmenting the narrow forehead requires an approach that can provide a more complete forehead-temporal type of augmentation.
Traditional methods of forehead augmentation, like bone cements, are ineffective for the too narrow forehead. By definition the bone cement must stay on the bone where it can bond to it. Keeping it restricted to that anatomic bony location will actually make the forehead look more narrow and create a pseudo bossing effect. (increasing projection with no width increase)
Only a custom implant design can create an effective forehead widening look as it allows the implants to safely cross the temporal line and rest on the deep temporal fascia. How far done along the temporal area it should go depends on the perceived temporal deficiency. With the implant laying on the deep temporal fascia it can extend all the way down to the zygomatic arch level. A computer design also provides control of the various implant thicknesses across a broad area as well as its overall shape…which will be somewhat different between men and women.
Case Study: This female was bothered by the narrow shape of her forehead and temporal areas. She also wanted a bit more of a brow bone presence.
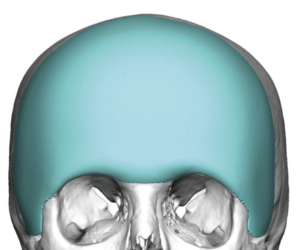
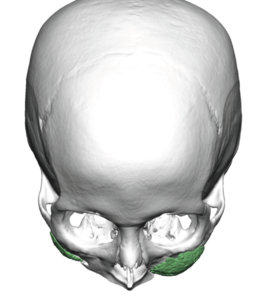
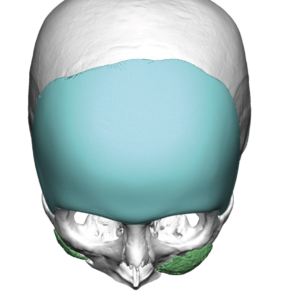 Using her 3D CT scan a total forehead-temporal implant was designed to provide widening to her forehead that extended down along the anterior temporal regions. Coverage was also extended to the brow bone areas.
Using her 3D CT scan a total forehead-temporal implant was designed to provide widening to her forehead that extended down along the anterior temporal regions. Coverage was also extended to the brow bone areas.
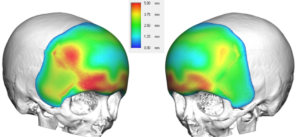 Nowhere was the implant designed to be any thicker than 5mms. It is important to be vigilant that as a bilateral implant and the large surface area that it covered, its volumetric effect (55ccs) is a lot more substantial than a simple linear measurement would lead one to believe.
Nowhere was the implant designed to be any thicker than 5mms. It is important to be vigilant that as a bilateral implant and the large surface area that it covered, its volumetric effect (55ccs) is a lot more substantial than a simple linear measurement would lead one to believe.



 Its surgical placement was done through a relatively small scalp incision aided by endoscopic release along the brow bone and lateral orbital rims. The temporal wings of the implant were placed in a subfascal position on top of the muscle to prevent any risk of implant edge visibility in the thinner tissues of the female temporal region.
Its surgical placement was done through a relatively small scalp incision aided by endoscopic release along the brow bone and lateral orbital rims. The temporal wings of the implant were placed in a subfascal position on top of the muscle to prevent any risk of implant edge visibility in the thinner tissues of the female temporal region.
 Her immediate intraoperative results showed a visible but not overdone forehead-temporal widening effect.
Her immediate intraoperative results showed a visible but not overdone forehead-temporal widening effect.
 To create a smooth and effective forehead widening effect, the augmentation must extend onto the temporal region. How far down along the temporal area it needs to go varies based on the degree of temporal narrowing. Such a large surface area forehead implant often looks like a partial helmet…which speaks to why large surface area coverages are needed in many types of skull augmentations. The implant design may look peculiar to some but is what is needed to create a smooth and harmonious augmented shape.
To create a smooth and effective forehead widening effect, the augmentation must extend onto the temporal region. How far down along the temporal area it needs to go varies based on the degree of temporal narrowing. Such a large surface area forehead implant often looks like a partial helmet…which speaks to why large surface area coverages are needed in many types of skull augmentations. The implant design may look peculiar to some but is what is needed to create a smooth and harmonious augmented shape.
While the traditional full coronal scalp incision can be used to place such a large forehead-temporal implant, it can also be successfully placed with more limited scalp incisions aided by endoscopic dissections in critical areas.
Case Highlights:
1) The narrow forehead involves more than just the forehead bone but the temporal soft tissues as well.
2) Adequately widening the forehead requires a custom forehead-temporal implant design that provides a comprehensive augmentation effect.
3) A custom forehead-temporal implant can be placed through a scalp incision that is limited to between the temporal lines using endoscopic release along the superolateral orbital rims.
Dr. Barry Eppley
Indianapolis, Indiana