

Background: Traditional temporal augmentation surgery addresses the hollowing that occurs by the side of the eye outside the lateral orbital rim. (non-hair bearing skin) This is the most common temporal or side of the head deficiency which represents lack of adequate soft tissue (muscle or fat) which comprises the anterior temporal fossa. (concavity) Several types of standard temporal implants, placed in the subfascial location, that are available to augment the anterior hollows based on the location of the needed effect. Type 1 standard temporal implants augment the lower half while Type 2 standard temporal implants treats the entire vertical extent of the hollows.
While temporal hollows may be the most common aesthetic side of the head deficiency it is also limited to one area. More encompassing side of tune head deficiencies, better known as a narrow head shape, can also be patient concerns. These are more obvious deficiencies in that the head shape appears more narrow from the front and back views. The underlying anatomic deficiency is more bone-based than muscle and 3D skull CT scans will show a more inverted V-shaped from front to back.
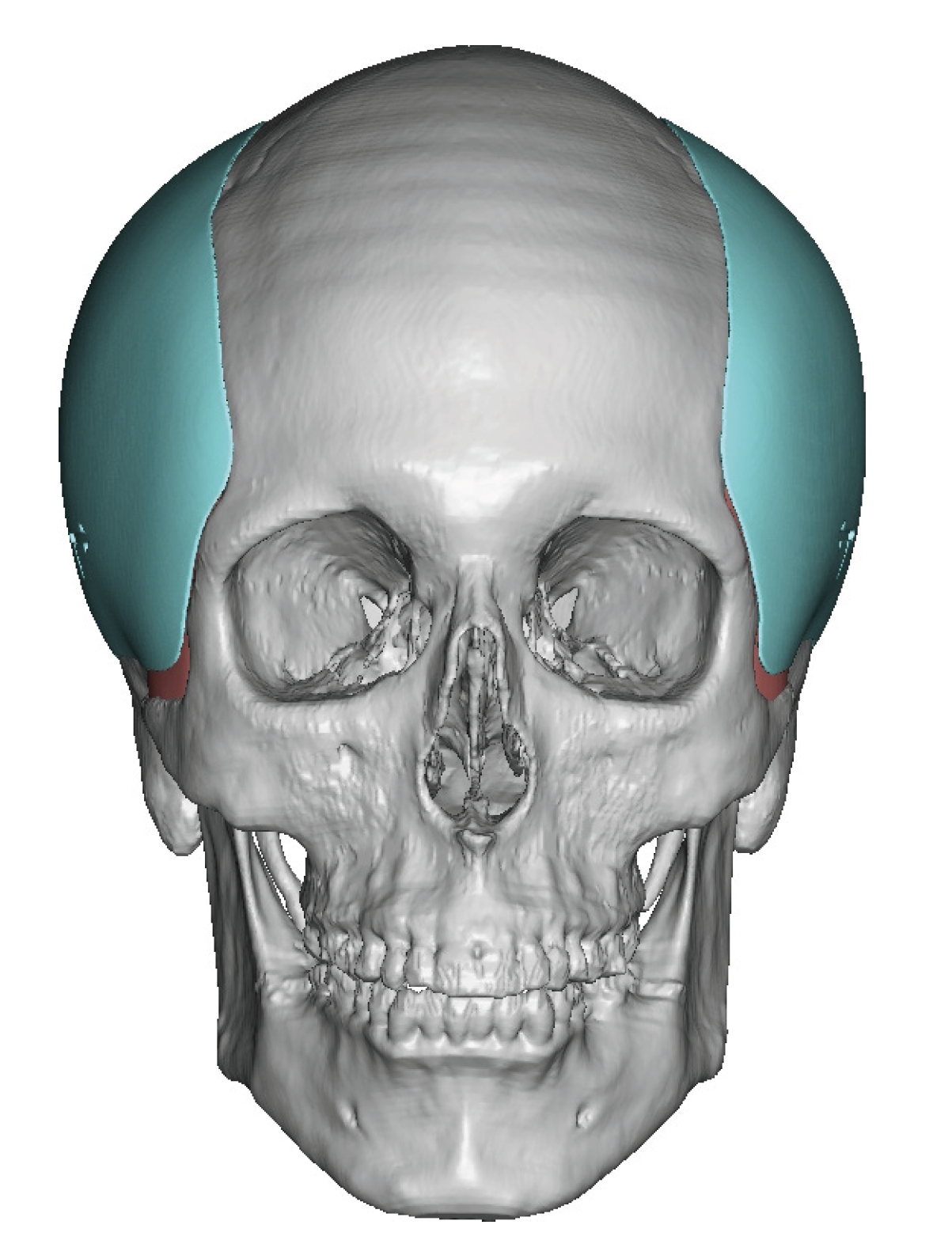
In diagnosing and treating these more extended temporal deficiencies I divide them into two types. Those that stay within the anterior, superior and posterior bony temporal lines is a Type 3 augmentation. (which means it is a total muscle enhancement) Those patients that need to provide an augmentation yup onto the bone beyond the bony temporal lines is a Type 4 temporal augmentation. ( which is a combined bone and muscle enhancements)
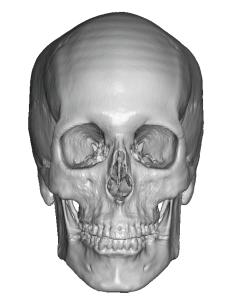
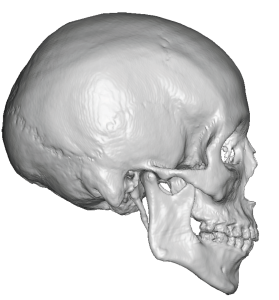 Case Study: This female had long been bothered by her narrow head shape. As a result she wore her hair in a way that made the sides of her head look fuller. Her 3D CT scan showed mild-moderate bony narrowing with a rounded temporal line and parasagittal skull angulations. In the side view the sagittal to temporal line distance was vertically elongated.
Case Study: This female had long been bothered by her narrow head shape. As a result she wore her hair in a way that made the sides of her head look fuller. Her 3D CT scan showed mild-moderate bony narrowing with a rounded temporal line and parasagittal skull angulations. In the side view the sagittal to temporal line distance was vertically elongated.
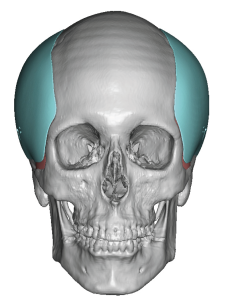
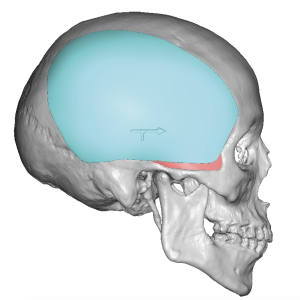 To provide her with a moderate increase in head (temporal) width custom temporal implants were designed to provide full muscular augmentation. Maximum implant thickness located above the ears was 6mms. The bilateral implants provided 95cc of volume.
To provide her with a moderate increase in head (temporal) width custom temporal implants were designed to provide full muscular augmentation. Maximum implant thickness located above the ears was 6mms. The bilateral implants provided 95cc of volume.

 Under general anesthesia and through postauricular sulcus incisions submuscular pockets were developed after passing through the deep temporal fascia. They implants were inserted, positioned and secured with a single microscrew.
Under general anesthesia and through postauricular sulcus incisions submuscular pockets were developed after passing through the deep temporal fascia. They implants were inserted, positioned and secured with a single microscrew.

 Closure was done over a drain in multiple layers with resorbable sutures.
Closure was done over a drain in multiple layers with resorbable sutures.

 The immediate increase in head width could be appreciated from the frontal view.
The immediate increase in head width could be appreciated from the frontal view.

 When seen the next day for head dressing and drain removals, an expected similar amount of head width increase was seen.
When seen the next day for head dressing and drain removals, an expected similar amount of head width increase was seen.
The concept of widening the narrow head by an implant placed under the temporal muscle is an extension of what was learned from the early efforts at more limited Type 1 and 2 standard temporal implants. Augmenting the size of the temporal muscle can be done by placing an implant either under (submuscular) or on top of the muscle. (subfascial) Each location has its advantages and disadvantages but in larger implants the tissues tolerances are better under the muscle with increased tissue coverage.
Key Points:
1) The narrow head can be widened by a variety of temporal implant concepts which differ based on the front to back length of the desired augmentation effect.
2) In Type 3 temporal augmentation the submuscular implant location is chosen for head widening that stays inside the bony temporal line.
3) Type 3 custom temporal implants are inserted through postauricular sulcus incisions which offer essentially scarless surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon