


Background: The anterior branch of the superficial temporal artery is the only portion of the external carotid system that can become externally visible. As it leaves the temporal hairline and crosses into the side of the forehead its pathway is superficial above the deep temporal fascia. If the artery becomes enlarged, due to a medical condition (e.g., temporal arteritis) or other benign but unknown reasons, it becomes visible. It creates a classic serpiginous appearance in this visibility which is essentially recognizable.
While some people have continuous or intermittent prominent temporal arteries that do not bother them, others consider them aesthetically undesirable and seek treatment for them. The vast majority of these patients are men who are more prone to this aesthetic temporal issue. This is presumably due to larger temporal arteries with thicker muscular walls. Most females have smaller temporal arteries with thinner muscular walls which makes them less susceptible. There may also be some hormonal influences contributing to these differences but this is yet unknown.
But females do occasionally present with prominent temporal arteries and they typically are thin. Their histories are similar in that they have spontaneously appeared with no known inciting event. When appearing in women they are more aesthetically disturbing perhaps because it is a more masculine feature based on its more common occurrence in men.
 Case Study: This female presented with very prominent temporal arteries with the right larger than the left. Its course could be seen to not be the typical enlarged anterior branch of the superficial temporal artery. Rather it came off of the main trunk of the temporal artery in front of the ear well below the Y-split of the anterior and posterior branches. I will call this an accessory branch off of the main temporal artery trunk.
Case Study: This female presented with very prominent temporal arteries with the right larger than the left. Its course could be seen to not be the typical enlarged anterior branch of the superficial temporal artery. Rather it came off of the main trunk of the temporal artery in front of the ear well below the Y-split of the anterior and posterior branches. I will call this an accessory branch off of the main temporal artery trunk.
 Preoperatively four ligation sites were marked along its course on each side.
Preoperatively four ligation sites were marked along its course on each side.

 Under local anesthesia on the right side the four ligation points were opened, the artery dissected out and double ligation done with 5-0 blue prolene. In checking with the doppler the arterial signal was not completely eliminated. The signal was trace out and a fifth ligation site was done. This then eliminated the doppler signal.
Under local anesthesia on the right side the four ligation points were opened, the artery dissected out and double ligation done with 5-0 blue prolene. In checking with the doppler the arterial signal was not completely eliminated. The signal was trace out and a fifth ligation site was done. This then eliminated the doppler signal.

 From what was learned on the right side on the left side only four ligations sites were done to eliminate the arterial signal. The proximal ligation site for the accessory branch was done at the low end of the temporal hairline.
From what was learned on the right side on the left side only four ligations sites were done to eliminate the arterial signal. The proximal ligation site for the accessory branch was done at the low end of the temporal hairline.
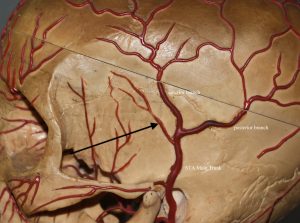 While prominent temporal arteries are often attributed to the anterior branch of the superficial temporal artery, in many cases that is not anatomically correct. As seen in this female the prominence is a branch that comes off the main trunk of the temporal artery long before it’s Y-split into anterior and posterior branches. This branch of the temporal artery is either often not shown in anatomic illustrations or it is shown a small trivial branch. But when it becomes enlarged it is feed directly from the main temporal trunk and its diameter expands considerably. For ligations to be successful the most proximal ligation must be closer to the main trunk. Unless it it ligated there the signal will not be eliminated no matter how many more distal ligations are done.
While prominent temporal arteries are often attributed to the anterior branch of the superficial temporal artery, in many cases that is not anatomically correct. As seen in this female the prominence is a branch that comes off the main trunk of the temporal artery long before it’s Y-split into anterior and posterior branches. This branch of the temporal artery is either often not shown in anatomic illustrations or it is shown a small trivial branch. But when it becomes enlarged it is feed directly from the main temporal trunk and its diameter expands considerably. For ligations to be successful the most proximal ligation must be closer to the main trunk. Unless it it ligated there the signal will not be eliminated no matter how many more distal ligations are done.
Case Highlights:
1) Prominent temporal arteries are seen far less frequently in women than men.
2) Multi-level temporal artery ligations adios the same in both men and women.
3) The use of doppler ultrasound testing provides the most useful intraoperative for the number and location of the temporal artery ligation sites.
Dr. Barry Eppley
World-Renowned Plastic Surgeon