

Background: The flat back of the head is one of the common aesthetic skull deformities. It usually originates from either a genetic predisposition or a deformational effect of in utero or post birth head positioning. (occipital plagiocephaly) The flatness can be on just one side or both. (bilateral) When it occurs bilaterally there are aesthetic issues of skull disproportion that often bothers the person enough that they may great efforts at camouflaged by various hairstyles and hat wear.
Cosmetic correction of the flat back of the head is done using a variety of onlay implant materials. The contour of the bone is expanded through subperiosteal augmentation whose amount is controlled by the ability of the overlying scalp to expand.Those materials that are applied and shaped intraoperatively are several types of bone cements. (PMMA and hydroxyapatite cement) Preformed custom occipital implant materials include silicone, Medpor, HTR and PEEK. Of these custom shaped materials, only silicone is soft and flexible while the other polymers are quite rigid.
 HTR (Hard Tissue Replacement) is a well known cranioplasty material. It has been used as a custom made implant for cranial defects for over 25 years. It is a unique polymer material because it is both porous and hydrophilic. These material characteristics allow it to become well vascularized throughout its thickness after implantation. It has a very successful history of inlay reconstructive use for skull bone defects but has been very rarely used as an onlay material for aesthetic augmentation.
HTR (Hard Tissue Replacement) is a well known cranioplasty material. It has been used as a custom made implant for cranial defects for over 25 years. It is a unique polymer material because it is both porous and hydrophilic. These material characteristics allow it to become well vascularized throughout its thickness after implantation. It has a very successful history of inlay reconstructive use for skull bone defects but has been very rarely used as an onlay material for aesthetic augmentation.
Case Study: This 38 year-old male had a very flat back of the head for which he had prior attempts at occipital augmentation. He had a prior occipital implant (material unknown) placed through a long coronal scalp incision which ultimately became infected and had to be removed. This left the back of his scalp scarred and more rigid than normal. He thoughtfully considered all the implant materials and chose HTR because of its potential to become vascularized throughout the material. A 3D CT scan was used to create an occipital implant design of 18mm thick at its central portion.
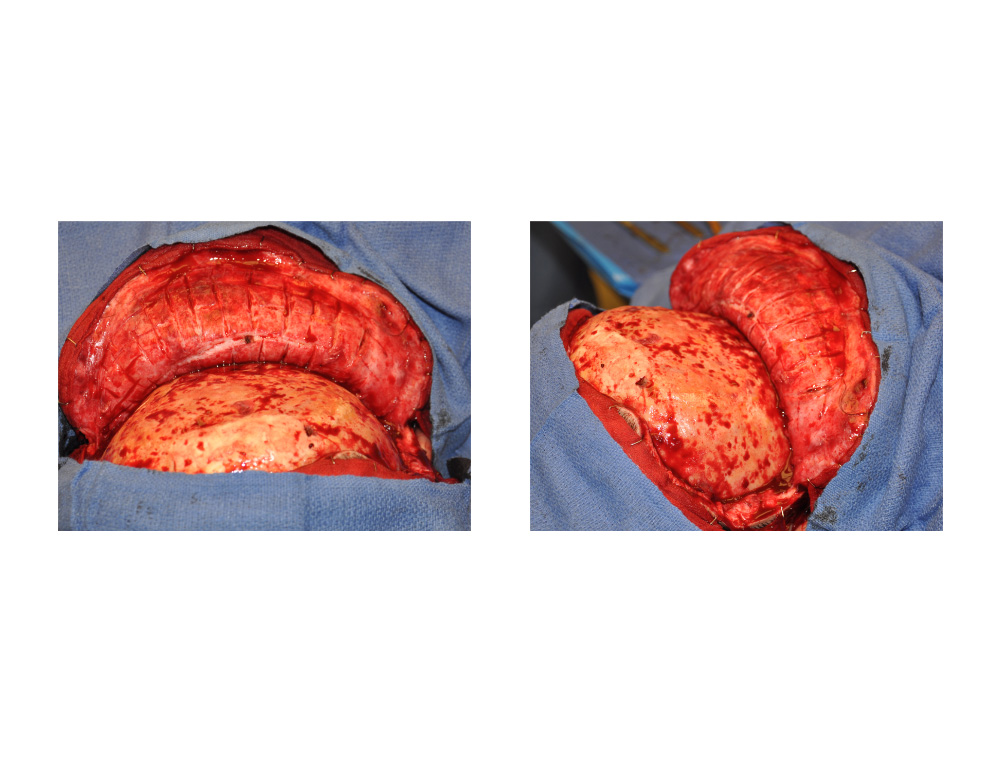 In the prone position under general anesthesia, his original high occipital scar was completely cut out down to the bone. An occipital scalp flap was developed down to below the nuchal ridge at the base of the occipital bone. While the scalp flap raised easily it was very thick and inflexible. Extensive cross cuts in a grid pattern were done through the scar to create a full occipital flap release to create enough tissue looseness to close over an implant augmentation.
In the prone position under general anesthesia, his original high occipital scar was completely cut out down to the bone. An occipital scalp flap was developed down to below the nuchal ridge at the base of the occipital bone. While the scalp flap raised easily it was very thick and inflexible. Extensive cross cuts in a grid pattern were done through the scar to create a full occipital flap release to create enough tissue looseness to close over an implant augmentation.
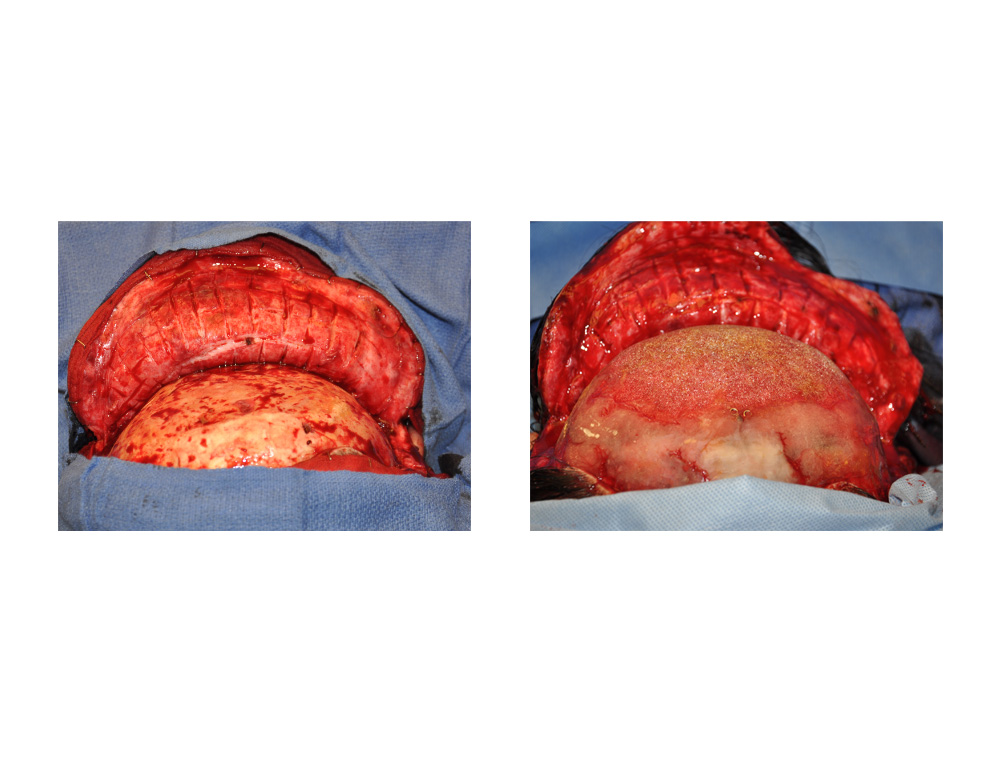
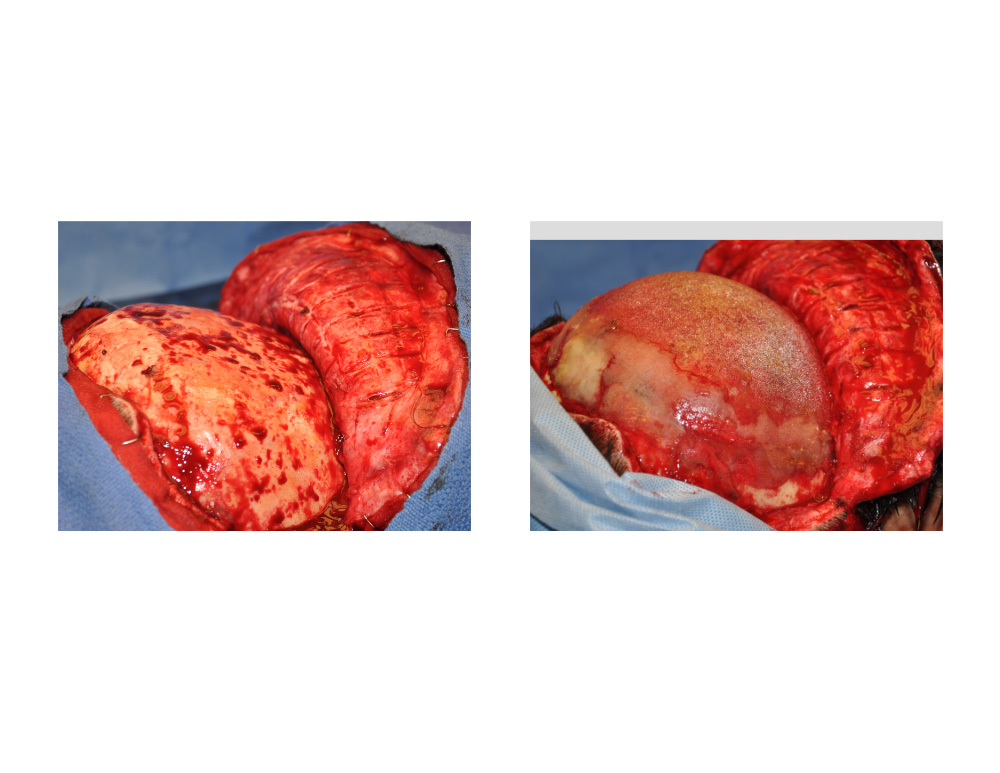
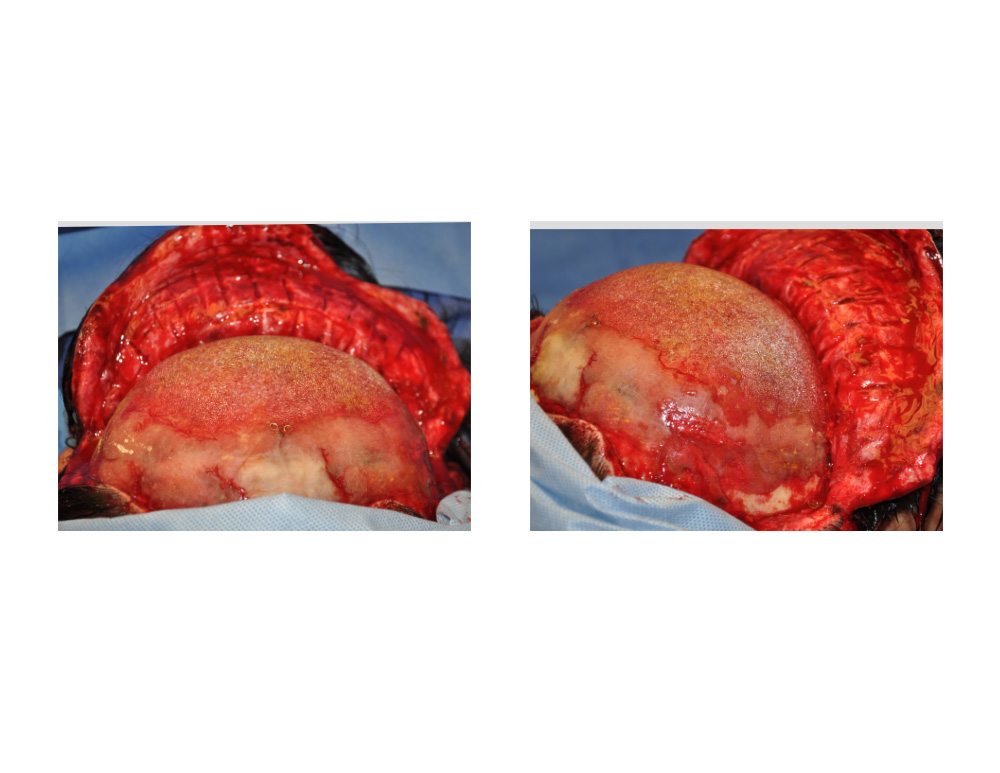 The HTR occipital implant was soaked in antibiotic solution and placed in its proper position on the position. It was secured with small plates and screws in a triangular pattern. Because the edge of the HTR material can not be made paper thin, a layer of PMMA bone cement was used to create a smooth transition from the implant to the bone.
The HTR occipital implant was soaked in antibiotic solution and placed in its proper position on the position. It was secured with small plates and screws in a triangular pattern. Because the edge of the HTR material can not be made paper thin, a layer of PMMA bone cement was used to create a smooth transition from the implant to the bone.
 With an 18mm expansion in a previously operated and scarred flap, even with using a full coronal incision, the wound closure was tight over the implant. Fortunately no wound separation developed when the staples were removed. He went on to heal uneventfully, has developed no infection or fluid collections and is satisfied with his results.
With an 18mm expansion in a previously operated and scarred flap, even with using a full coronal incision, the wound closure was tight over the implant. Fortunately no wound separation developed when the staples were removed. He went on to heal uneventfully, has developed no infection or fluid collections and is satisfied with his results.
Rigid implant materials like HTR can be successfully used in aesthetic skull augmentations. But the material characteristics makes for the need to use a long scalp incision for placement and some experience on knowing how to properly secure it without fracture or palpable implant edges.
Case Highlights:
1) Occipital augmentation skull reshaping surgery can be done by custom implant materials like HTR which is also porous.
2) Because HTR is a hard inflexible material it must be placed through a full coronal scalp incision.
3) Fine edging of HTR as an onlay material may need to be supplemented with a bone cement material to create perfectly smooth edge transitions.
Dr. Barry Eppley
Indianapolis, Indiana