

Background: Undereye hollows are a not uncommon aesthetic midface concern.They are seen in two basic types of patients. In the older patients undereye hollows occur from aging with loss of fat from underneath the lower eyelid and inferior orbital compartments. It may also be caused from a prior lower blepharoplasty where excessive fat has been removed. In these patients the underlying bone (infraorbital-malar complex) has normal projection. Conversely in the younger patient undereye hollows occur because the infraorbital-malar complex lacks adequate forward projection. This creates the classic negative orbital vector.
In congenital undereye hollows the appearance of the eye and lower eyelids is affected due to the lack of bony support. The eye may appear to be bulging and the downslanrting lower eyelid allows for excessive scleral show which contributes to the pseudoproptotic eye appearance. The inferior and lateral cheekbone will have inadequate forward projection as it is attached and correlates with the shape of the infraorbital rim. It may also have lack of lateral cheek projection as well.
The infraorbital-malar skeletal deficiency may be thought of like the zygomaticomaxillary complex (ZMC) is in facial fracture repair. Adequate correction comes from rotating the ZMC complex upon and out from its displacement down into the maxillary sinus. Similarly good correction of under eye hollows comes from ‘rotating’ the deficient infraornital-malar complex (IOM) up and out eliminating the negative orbital vector and improving eye and lower eyelid support. Trying to do bony repositoning has practical limitations so the best and most effective approach is custom infraorbital-malar (IOM) implants.

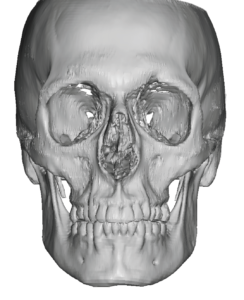 Case Study: This patient desired to have their undereye hollows and eye appearance improved. Their 3D CT scan showed a recessed infraorbital rim and anterior malar bones. (compared to the projection of the supraorbital rim. The infraorbital rim showed a low swooping rim shape with the right lower than the left.
Case Study: This patient desired to have their undereye hollows and eye appearance improved. Their 3D CT scan showed a recessed infraorbital rim and anterior malar bones. (compared to the projection of the supraorbital rim. The infraorbital rim showed a low swooping rim shape with the right lower than the left.
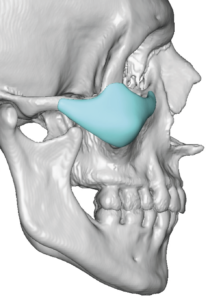
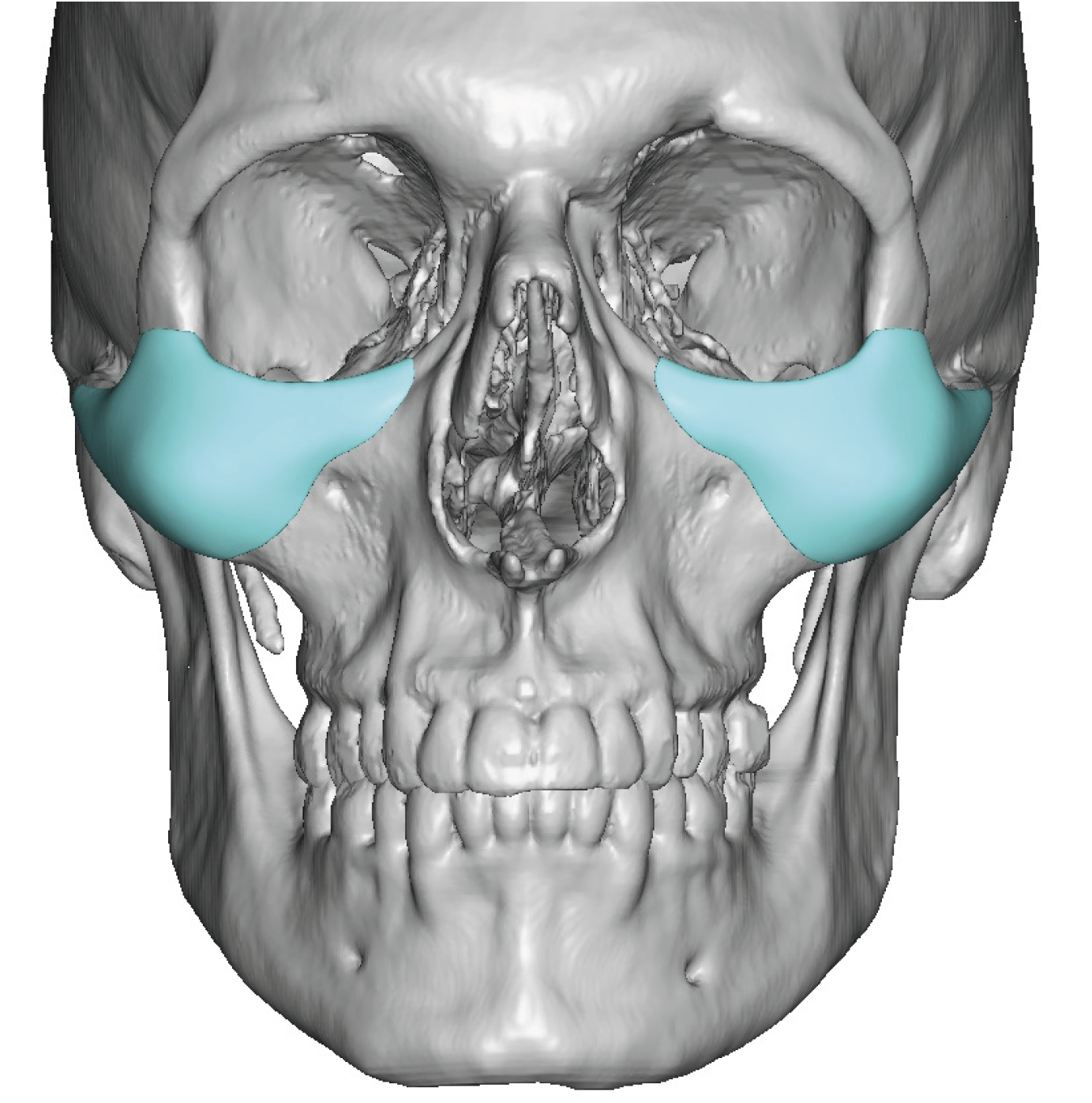
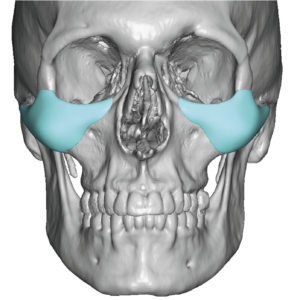 Custom Infraorbital-malar implants were designed to saddle and build up the infra orbital rims as well as provide substantial increased projection of the cheekbone. In essence a new overlay infraorbital-malar complex was designed to built out the deficiency.
Custom Infraorbital-malar implants were designed to saddle and build up the infra orbital rims as well as provide substantial increased projection of the cheekbone. In essence a new overlay infraorbital-malar complex was designed to built out the deficiency.
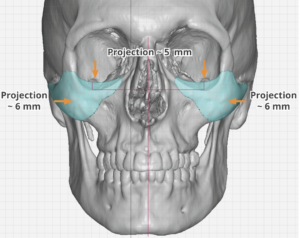 The saddling of the infraorbital rim of the implant was substantial at 5mms and the increased cheek projection was 6mms.
The saddling of the infraorbital rim of the implant was substantial at 5mms and the increased cheek projection was 6mms.

![]() Under general anesthesia the custom IOM implants were placed through limited lower eyelid incisions. Once the implants were placed and secured with a single fixation screw per side, double lateral canthoplasties were performed with Alloderm lower eyelid spacer grafts.
Under general anesthesia the custom IOM implants were placed through limited lower eyelid incisions. Once the implants were placed and secured with a single fixation screw per side, double lateral canthoplasties were performed with Alloderm lower eyelid spacer grafts.



 At four months postop he had substantial improvement in the elimination of the undereye hollows and more horizontal leveling of his lower eyelids.
At four months postop he had substantial improvement in the elimination of the undereye hollows and more horizontal leveling of his lower eyelids.
Significant undereye hollows are a skeletal deficiency problem for which custom IOM implants provide the 3D augmentation needed to change a negative orbital vector into at least a neutral one. But the implant augmentation alone can not guarantee elevation of the lower eyelid. Complementary procedures to the IOM implant are needed which are lateral canthoplasties and lower eyelid spacer grafts. Not only will these procedures decrease the risk of postoperative ectropion they provide greater assurance that some improvement on the low position will be achieved.
Case Highlights:
1) Congenital undereye hollows are caused by a developmental deficiency of the infraorbital rim and anterior malar bones.
2) Custom infraorbital-malar implants provide the definitive correction for undereye hollows that is far superior to fillers or fat injections.
3) While custom infraorbital-malar implants improves the bony deficiency additional lower eyelid suspension procedures are also needed correct the shape of the lower eyelid.
Dr. Barry Eppley
World-Renowned Plastic Surgeon