

Background: Large augmentative skull implants are indicated when there is a congenitally head shape deformity that lacks height as well as width. When these dimensional increases are significant such cases almost always requires a first stage scalp expansion or having had a prior skull implant in place. Despite the relatively large size of the implant it is generally very well tolerated and complications are very few. The extra cranial onlay site is a very privileged implantation area due to the superb blood supply of the scalp and its low infectivity risks.
Despite the favorable features of skull augmentation site, whether it be bone or on top of the deep temporal fascia, the operation must still be performed in an aesthetic fashion. This means that the scalp incision to place it must not be an aesthetic distraction in length or location and the implant must be able to be passed through it for placement. There is also the need to be able to properly position the implant as per the preoperative design to achieve a symmetric result.
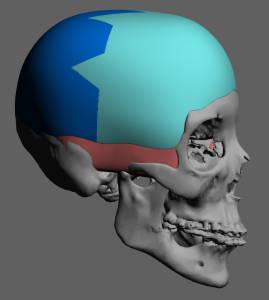
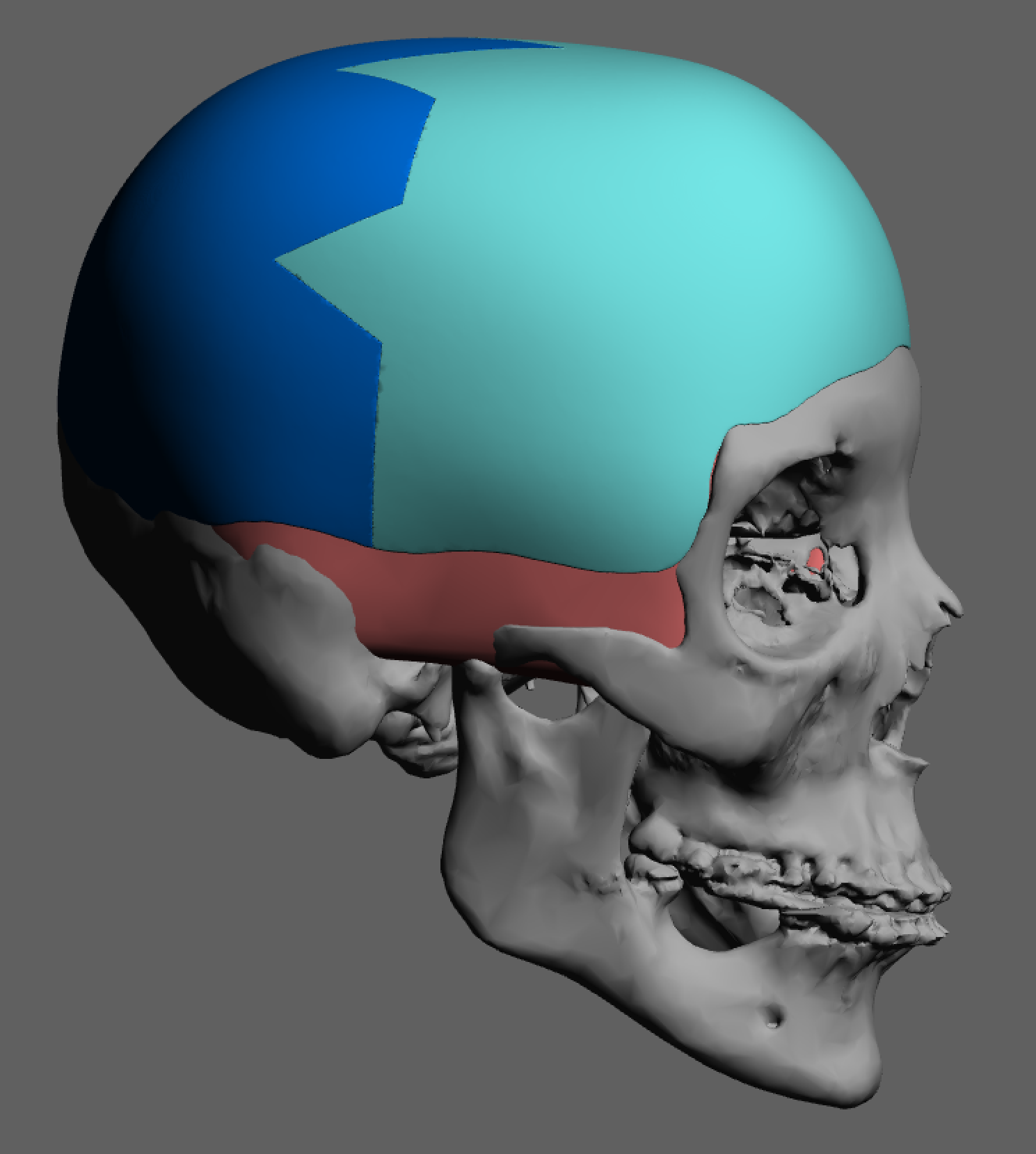
 Case Study: This female had a prior history of a two stage skull augmentation to treat what was a very flat head on top which was also very narrow from side to side. This was particularly seen in the very narrow and backwardly sloped forehead. While she achieved a marked improvement with the original 311cc skull implant, ideal forehead and temporal width was not fully achieved. A new custom skull implant was designed that kept the same sagittal height but provided additional width along the sides and also lowered the implant position down to the brow bones and inferior anterior temporal area. The new total implant volume was 371cc. The new implant was designed in a two piece fashion that fit together in a sharply angled saw tooth pattern.
Case Study: This female had a prior history of a two stage skull augmentation to treat what was a very flat head on top which was also very narrow from side to side. This was particularly seen in the very narrow and backwardly sloped forehead. While she achieved a marked improvement with the original 311cc skull implant, ideal forehead and temporal width was not fully achieved. A new custom skull implant was designed that kept the same sagittal height but provided additional width along the sides and also lowered the implant position down to the brow bones and inferior anterior temporal area. The new total implant volume was 371cc. The new implant was designed in a two piece fashion that fit together in a sharply angled saw tooth pattern.

 The skull implant replacement surgery was done through an extended sagittal scalp incision that was aided by the part she conveniently placed in her hair. A close up view of her prior sagittal scalp incision shows how well it had initially healed.
The skull implant replacement surgery was done through an extended sagittal scalp incision that was aided by the part she conveniently placed in her hair. A close up view of her prior sagittal scalp incision shows how well it had initially healed.
 Opening up the healed sagittal scalp incision showed how thick her scalp is and how far below the hair follicles the location of the implant and its capsule lies.
Opening up the healed sagittal scalp incision showed how thick her scalp is and how far below the hair follicles the location of the implant and its capsule lies.



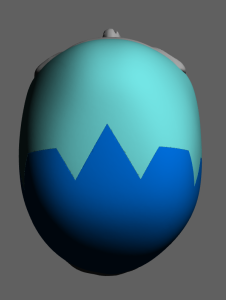
 The two-piece skull implant had a side to side split design with sharply angled interdigitating connections between the two pieces. This not only allowed for a precise fit to be obtained but eliminated any risk of a side to side shift malposition of the two implant pieces. Their placement on the patient’s scalp showed their indwelling location as well as the sequence in which they were placed.
The two-piece skull implant had a side to side split design with sharply angled interdigitating connections between the two pieces. This not only allowed for a precise fit to be obtained but eliminated any risk of a side to side shift malposition of the two implant pieces. Their placement on the patient’s scalp showed their indwelling location as well as the sequence in which they were placed.

 The front half of the implant was initially placed and secured into position with two percutaneous screws placed in the high temporal regions to the bone. The back of the implant was placed, fit tightly into the zigzag interface with the front half and secured with two screws.
The front half of the implant was initially placed and secured into position with two percutaneous screws placed in the high temporal regions to the bone. The back of the implant was placed, fit tightly into the zigzag interface with the front half and secured with two screws.



 In evaluating her original preoperative front view, the desired he’d widening effect from the forehead on back was achieved. When the forehead becomes wider its vertical inclination must also be increased for a proportionate change.
In evaluating her original preoperative front view, the desired he’d widening effect from the forehead on back was achieved. When the forehead becomes wider its vertical inclination must also be increased for a proportionate change.
Major head reshaping requires an augmentation that sits on bone as well as the soft tissue on the sides of the head. The skull implant and the material in which it is composed must be capable of covering that large skull surface area as well as able to be inserted and positioned through an acceptable scalp incisional length. The implant design mist also plan for a volume in which the scalp can comfortably close over it. Even with an implant volume over 300ccs all of these criteria can be met with the use a split design that is reassembled once inside the patient.
Case Highlights:
1) Large custom skull implants essentially augment all five head surfaces to some degree.
2) If the scalp has been adequately expanded, skull implant volumes over 300ccs can be safely accommodated.
3) A sagittally oriented scalp incision can be used for placement which has some advantages for anterior posterior pocket dissection.
4) Regardless of the incision type insertion is most effectively done using a split or two piece skull implant design.
Dr. Barry Eppley
Indianapolis, Indiana