

Background: Asymmetries in the shape of the head are not uncommon and come in a wide variety of types. One not uncommon type is that which affects the side of the head and is most noticeable to the patient in the front view. One side of the head sticks out further than the other. Usually the slimmer or more narrow side is preferred. The excessive often has a greater convex shape than the other side. It bowes out most above the ear.
While most think this is caused by an underlying thickness of bone it is most commonly due to an excess of muscle. The thickness of the temporal muscle on the side of the head is under appreciated. While the muscle is not as thick as it is in the temporal fossa area by the side of the eye, it is still thick enough that it usually shares an equal thickness as that of the temporal bone beneath it. When in doubt check a CT scan to assess the ratio of the muscle to bone between the two sides of the head. On a practical basis muscle removal from the side of the head can be done in a more scarless fashion than bone removal. While muscle removal can be done through an incision placed in a crease behind the ear, bone removal requires an incision up along the side of the head.
When it comes to temporal muscle reductions there are multiple techniques based on location or extent (posterior vs anterior) as well as amount. (partial vs total)
Case Study: This male had a left side of the head asymmetry with greater convexity of the temporal region above the ear than the other side. When he opened his mouth widely the left temporal area reduced/thinned, confirming that muscle reduction would be beneficial for symmetry improvement.
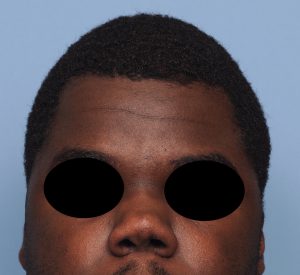
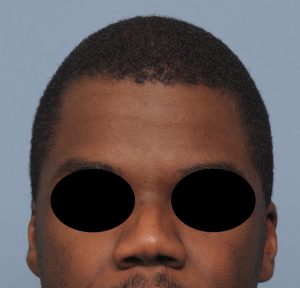 Under general anesthesia and through an incision placed in the crease behind his left ear (postauricular sulcus) the posterior temporal muscle was partially excised and transposed inferiorly to redistribute its mass. This created an immediate improvement in the symmetry of the two sides of the head which was maintained when seen one year later.
Under general anesthesia and through an incision placed in the crease behind his left ear (postauricular sulcus) the posterior temporal muscle was partially excised and transposed inferiorly to redistribute its mass. This created an immediate improvement in the symmetry of the two sides of the head which was maintained when seen one year later.

 The healing of the incision behind the ear was ‘scarless’ as it laid in the depth of the postauricular sulcus which makes it completely invisible. When folding the ear over a very fair scar could be seen.
The healing of the incision behind the ear was ‘scarless’ as it laid in the depth of the postauricular sulcus which makes it completely invisible. When folding the ear over a very fair scar could be seen.
While asymmetry of the side of the head can be caused by bone, which is very common in congenital plagiocephaly, in non-plagiocephaly side of the head asymmetries muscle reduction can provide an effective improvement. When done from an incision behind the ear, as most temporal reductions are done, the improvement in the asymmetry can truly be scarless.
Case Highlights:
1) Most non-plagiocephalic temporal or side of the head asymmetries have a significant muscle component to them.
2) In reducing a temporal asymmetry due to an excessive width/convexity, removal of the posterior portion of the temporalis muscle usually provides good improvement.
3) Temporal muscle removal offers a scarless approach to improving a side of the head asymmetry.
Dr. Barry Eppley
Indianapolis, Indiana