

Background: The most common chin reshaping procedure in a male is augmentation. Most commonly it is in a horizontal dimension but the chin augmentation changes may occasionally also include vertical lengthening and transverse widening. But regardless of the specific dimensional changes augmentation of the chin makes up 95% of all male requests/needs.
In women chin reshaping needs are quite different from men. Far more women request chin reduction than men and, in my experience, it is about a 50:50 mix of chin augmentations vs chin reductions in females. Part of this is that men can aesthetically tolerate a larger chin than women. Women may want a good jawline but they don’t want an overly prominent chin.
Men that present for chin reduction often have an overly large jaw and their chin reduction eventually comes from orthognathic surgery to set the entire lower jaw back. In my experience the most common dimensional change in male chin reduction is vertical. The entire face may look long but the lower facial third is often the most excessive due to a vertically long chin. In some of these longer chin men the mandibular plane angle is steep and the jaw angle is high, reflective of an abnormal vertical jaw growth pattern
In reduction of any vertically long chin the surgical options are a submental or intraoral technique. Each has their advantages and disadvantages but the bone reduction techniques are different. The submental approach shortens the chin bone by a horizontal ostectomy from the bottom part of the chin. The intraoral approach vertically shortens the chin by removal of a wedge of bone from its middle part. (wedge ostectomy) Besides the location of the scar the one major differences is in what happens to the chin pad soft tissues. In the submental technique a soft tissue excision is required as it has been freed from the bone. In the intraoral technique the soft tissue is naturally shortened due to its attachment to the inferior border of the chin bone which allows it to follow the bone superiorly.
Case Study: This male was bothered by his long vertical chin. He had a very steep mandibular plane angle and a high jaw angle position. Computer imaging demonstrated that vertical chin reduction produced a positive change in his facial proportions.
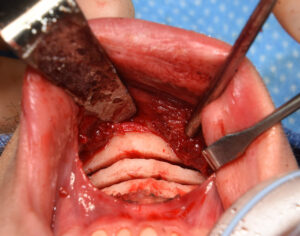
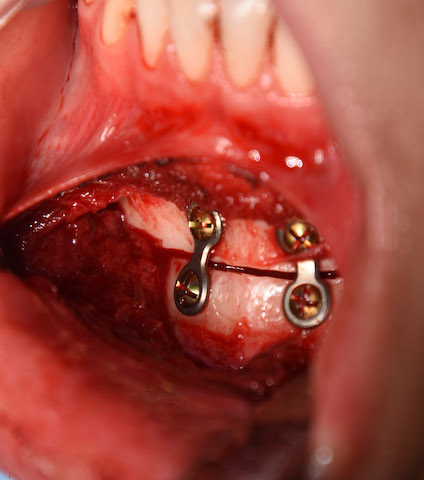
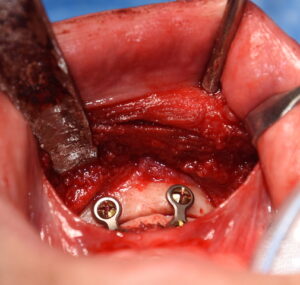 Under general anesthesia and through an intraoral approach, a 10mm (at the midline) wedge of bone was removed by double osteotomy cuts. Going out the sides the amount of bone removal became less to create a tapered bone removal so a large step off on the inferior border was prevented. The inferior down fractured chin segment was brought up and fixed with plates and screws to the superior chin segment.
Under general anesthesia and through an intraoral approach, a 10mm (at the midline) wedge of bone was removed by double osteotomy cuts. Going out the sides the amount of bone removal became less to create a tapered bone removal so a large step off on the inferior border was prevented. The inferior down fractured chin segment was brought up and fixed with plates and screws to the superior chin segment.


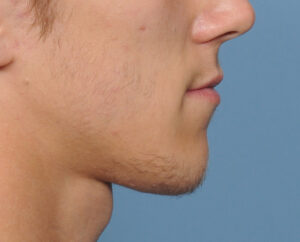
 At three months after surgery his results showed a visible vertical chin reduction with good bone healing and an uncomplicated recovery.
At three months after surgery his results showed a visible vertical chin reduction with good bone healing and an uncomplicated recovery.
 The intraoral vertical chin reduction technique allows for satisfactory lower facial shortening and avoids an external submental scar. Because the attached soft tissue chin pad follows the bone upward no apparent soft tissue redundancy (excess) usually occurs.
The intraoral vertical chin reduction technique allows for satisfactory lower facial shortening and avoids an external submental scar. Because the attached soft tissue chin pad follows the bone upward no apparent soft tissue redundancy (excess) usually occurs.
Case Highlights:
1) Chin reduction in a male is fairly rare with the need for vertical shortening as the most common reason to do so.
2) The intraoral method of isolated vertical chin reduction consists of an interpositional wedge osteotomy with inferior chin segment repositioning.
3) The attached soft tissue of the underside of the chin shortens with the superior bone repositioning.
Dr. Barry Eppley
Indianapolis, Indiana