

Background: An otoplasty procedure to setback protruding ears is the most common ear reshaping surgery and the second most performed aesthetic ear surgery. (earlobe repair/reconstruction is #1) It is a procedure that changes the shape of the cartilages that make up the structural rigidity of the ear. Many different types of cartilage manipulations have been described in the long history of such ear surgery all purporting to offer superior or more sustained results. But in the end almost any technique of cartilage reshaping can produce satisfactory results if performed well.
Every cartilage technique in otoplasty strives to pull the ear closer to the side of the head and involves either the concha, the anti helical fold or both cartilage locations. These are central or middle ear locations of pullback in which the superior ear and the lower earlobe are less affected. While there are additional techniques to address these other ear areas along with the central-based techniques in a setback otoplasty they can be either overlooked or under utilized. But even with their use if the central area is over pulled an over corrected or pulled back too far look can occur.
While there are numerous numerical assessments of how the ear should be ideally positioned on the side of the head (auriculocephalic angle) in the end how the patient sees its appearance is the most important aesthetic criteria. I have seen many patients with ears that may look out too far by the numbers or even too close to the side of the head in which patients are quite content. But the one feature of an ear that patients are least tolerant of is disruption or lack of a smooth outer helical rim. This is particularly so if they had one before any surgical manipulation.
In the over corrected ear the loss of a smooth and visible outer helical rim is its hallmark feature. If seen early suture release may correct it. But after the first month of surgery a surgical release will no longer be effective.
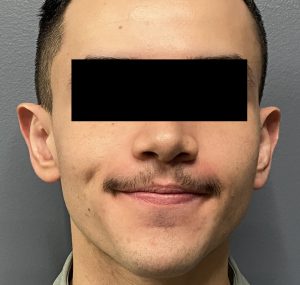
Case Study: This young male had an otoplasty 6 months previously which resulted in an undesired result. While the ear did stick out less the helical rim was not visible in the central part of the ear.

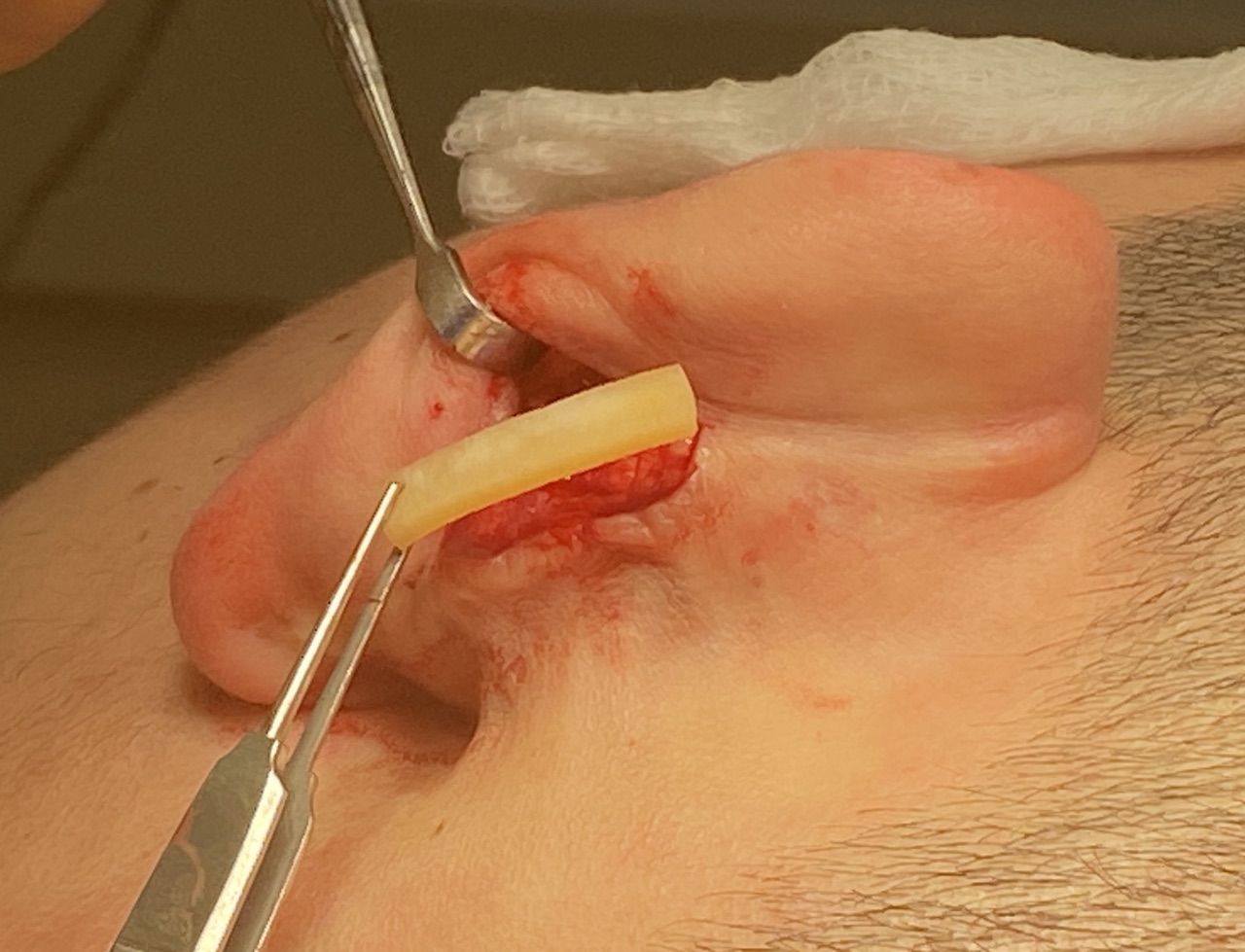
 Under local anesthesia and through the original postauricular incision the antihelical fold areas of each ear was released of all permanent sutures and the outer helical rims bent back out. Into the now more open antihelical fold area cadaveric rib cartilage grafts were placed to hold out the released helical rims
Under local anesthesia and through the original postauricular incision the antihelical fold areas of each ear was released of all permanent sutures and the outer helical rims bent back out. Into the now more open antihelical fold area cadaveric rib cartilage grafts were placed to hold out the released helical rims

 When seen six months later the helical rims had maintained their released position and the ears had a more confluent shape.
When seen six months later the helical rims had maintained their released position and the ears had a more confluent shape.
No matter what otoplasty technique is used it is an art form as to how it is applied. How much to pull the ears back and keeping the ear shape smooth and symmetric is prone to under- and over corrections. With an over correction it has to be caught very early for simple suture release to work. The ear cartilage loses memory quickly. Once this memory is lost cartilage needs to be added for the support needed for some amount of otoplasty reversal.
Key Points:
1) The most common area of the ear for overcorrection in setback otoplasty surgery is the middle or conchal ear area.
2) Unless a very early release is done within the first month after surgery overcorrection improvement will require a cartilage graft.
3) Postauriclar cartilage grafts can be placed either as a vertical strut or into the original released cartilage fold to help push the ear out.
Dr. Barry Eppley
World-Renowned Plastic Surgeon