


Background: Unlike a lack of horizontal projection a vertical deficiency of the chin is frequently undiagnosed or under diagnosed. This may be because the most common form of chin augmentation is an implant whose designs are intended for horizontal augmentation only. It may also be that the best option to most vertically deficient chins is an osteotomy, an operation not performed by many plastic surgeons.
The vertically short chin has many visible characteristics that goes beyond measuring the facial thirds. When the chin tis vertically short it essentially compresses the anterior lower third of the face. This creates the potential for a deep labiomental fold, an upturned soft tissue chin pad, an overbite, lower lip eversion and downturned mouth corners. These are the overall signs of too little space for the soft tissue and bony anatomy present.
Besides these physical findings the other way to determine of vertical lengthening is needed is computer imaging. Lengthening the chin digitally to varying degrees can help the patient determine if such a change is seen by them as beneficial. If so then the question is how much vertical lengthening is needed. There are several clinical maneuvers to help determine the vertical increase from a jaw thrust (open the jaw open until the length of the chin looks good and then measure the gap between the front teeth) and/or the placement of soft rubber wedges of varying thicknesses between the front teeth. These interincisal linear measurements correlate directly with the observable chin lengthening seen with their use.

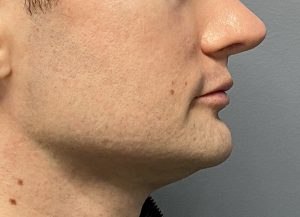 Case Study: This young male had many of the classic vertical short chin findings, deep labiomental fold, upturned chin pad and a flat mandibular plane angle. (Bottom of chin equal to same horizontal level as the jaw angles) Interincisal measurements showed that a 10mm increase made a pleasing change to his chin length.
Case Study: This young male had many of the classic vertical short chin findings, deep labiomental fold, upturned chin pad and a flat mandibular plane angle. (Bottom of chin equal to same horizontal level as the jaw angles) Interincisal measurements showed that a 10mm increase made a pleasing change to his chin length.

 Under general anesthesia and through an intraoral approach the chin bone was down fractured and plated with a 10mm opening gap between the bone edges. The bony gap was filled with wedges of cut cadaveric corticocancellous bone pieces.
Under general anesthesia and through an intraoral approach the chin bone was down fractured and plated with a 10mm opening gap between the bone edges. The bony gap was filled with wedges of cut cadaveric corticocancellous bone pieces.

 The immediate change in his chin length was apparent in comparing before and after chin profiles.
The immediate change in his chin length was apparent in comparing before and after chin profiles.

 Longer term results confirmed what was seen intraoperatively.
Longer term results confirmed what was seen intraoperatively.
Key Points:
1) The significantly vertically short chin has numerous characteristics beyond being less than a proportionate measured lower third of the face.
2) Lengthening the bone by an osteotomy and an interpostional graft is the best procedure for more than 5 or 6mms of needed chin length.
3) Th exact amount of vertical chin lengthening desired can be preoperatively determined by a visualized jaw thrust and/or interincisal wedges.
Dr. Barry Eppley
World-Renowned Plastic Surgeon