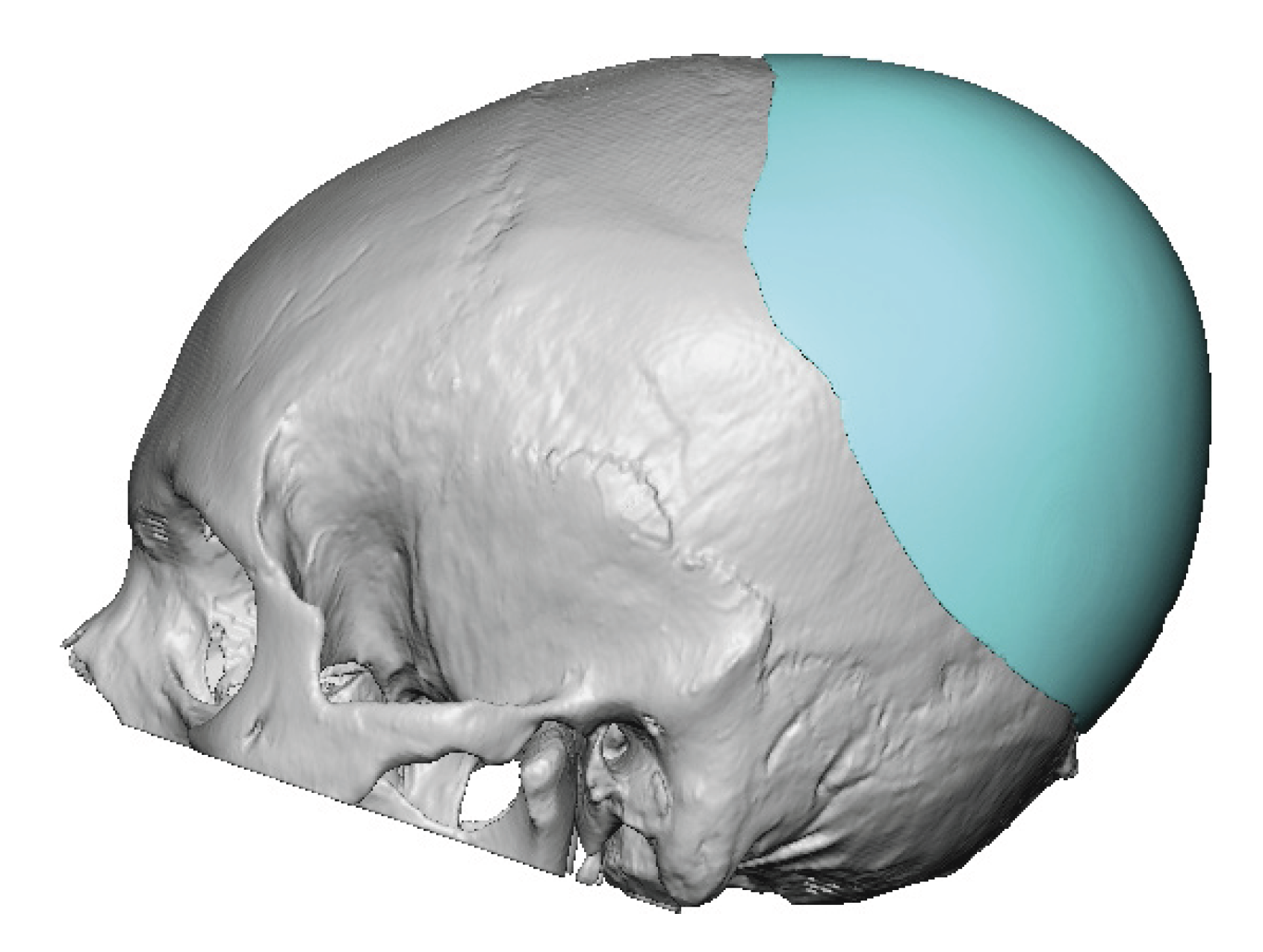


Background: One of the most areas of skull augmentation is the back of the head. Plagiocephaly (flatness on one side), brachycephaly (flatness on both sides) and posterior fontanelle depressions are the most common reasons people seek an improved and more symmetric outward contour augmentation. The most reliable and effective method of such skull augmentations is with a custom skull implant where the surface area coverage, thicknesses and a smooth outer contour can be completely controlled by the preoperative design process.
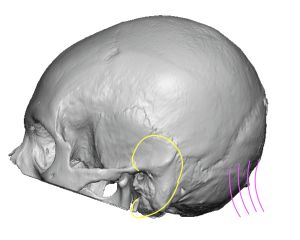 When augmenting the back of the head one important consideration often overlooked is where the skeletal back of the head actually is. Most people do not realize how high the back of the skull is located. As a general rule the lower end of the back of the head, where the strong neck muscles attach, is about at the same level as the top of the ear. (yellow = ear, purple = neck muscles) Another way to realize its location is the back of the head is at the same level as that of forehead on the front of the skull. Their slopes and projection may be different but the front and back of the head are equal in position.
When augmenting the back of the head one important consideration often overlooked is where the skeletal back of the head actually is. Most people do not realize how high the back of the skull is located. As a general rule the lower end of the back of the head, where the strong neck muscles attach, is about at the same level as the top of the ear. (yellow = ear, purple = neck muscles) Another way to realize its location is the back of the head is at the same level as that of forehead on the front of the skull. Their slopes and projection may be different but the front and back of the head are equal in position.
As a result setting the maximum projection of the back of head needs to take into consideration how low the augmentation needs to be. The strong attachments of the neck muscles at the bottom of the visible occipital bone serve as the inferior limit of the augmentation in most patients. But in the instances of when the augmentation needs to be lower extending onto the muscle fascia can be considered.
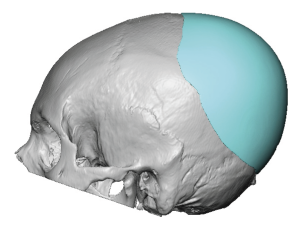 Case Study: This male desired to have the back of his head augmented. He has been ridiculed for the flatness on the back of his head and he always wore his hair long to hide it. But he now decided to undergo an augmentation to change his long term concern about the shape of his head. Using his 3D CT scan a custom implant was designed with 13mm projection and a volume of 125ccs. The planned incision was to use an existing low horizontal scalp crease.
Case Study: This male desired to have the back of his head augmented. He has been ridiculed for the flatness on the back of his head and he always wore his hair long to hide it. But he now decided to undergo an augmentation to change his long term concern about the shape of his head. Using his 3D CT scan a custom implant was designed with 13mm projection and a volume of 125ccs. The planned incision was to use an existing low horizontal scalp crease.

 The implant was designed with internal wedges to aid its insertion through the incision. Perfusion holes of 5mm diameter were placed around its perimeter to aid postoperative tissue ingrowth.
The implant was designed with internal wedges to aid its insertion through the incision. Perfusion holes of 5mm diameter were placed around its perimeter to aid postoperative tissue ingrowth.

 Under general anesthesia and in the prone position an incision was made in the low scalp skin crease. Through which subperiosteal dissection was done from the nuchal ridge up onto the top and sides of his head. The implant was inserted and to get it properly positioned dissection was carried onto the neck muscle fascia.
Under general anesthesia and in the prone position an incision was made in the low scalp skin crease. Through which subperiosteal dissection was done from the nuchal ridge up onto the top and sides of his head. The implant was inserted and to get it properly positioned dissection was carried onto the neck muscle fascia.
 A two layer scalp closure was then done over a drain.
A two layer scalp closure was then done over a drain.

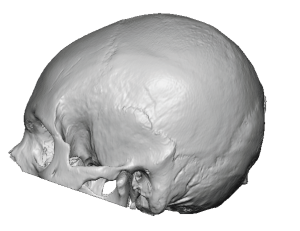
 His head dressing and drain were removed the next day where the improvement in the shape of the back of his head could readily be seen.
His head dressing and drain were removed the next day where the improvement in the shape of the back of his head could readily be seen.
When augmentation the back of the head is considered and an implant designed to augment it the first consideration is what is the vector of the maximum projection that is needed. The more horizontal the projection is the lower the edge of the implant needs to go to keep a good head shape in profile. If needed the implant may have to be positioned with its lower edge past the nuchal ridge onto the neck muscle fascia. As long as it does not extend too far onto the neck fascia it should not cause any discomfort with significant neck extension.
Key Points:
1) Back of the head augmentations are best done with a custom skull implant design for both the largest and smoothest contour change.
2) The lowest possible scalp incision is used in the back of the head, preferably a horizontal scalp indentation if it exists.
3) To get the implant as low as possible it may be necessary to place its lower edge below the bone edge onto the muscle fascia.
Dr. Barry Eppley
World-Renowned Plastic Surgeon